Methylmalonic Acidemia (MMA) is a rare and lethal inborn error of metabolism (IEM) that typically first with onset in infancy or early childhood, with a high mortality rate and poor long-term prognosis [2]. The condition is caused by mutations in the methylmalonyl-CoA mutase (MCM) gene or its cofactor, adenosylcobalamin (AdoCbl), leading to disruptions in the metabolic pathways of propionic acid precursor amino acids (valine, isoleucine, threonine, methionine), as well as propionate, odd-chain fatty acids, and cholesterol side chains. These disruptions result in the abnormal accumulation of 3-hydroxypropionic acid, methylcitric acid, and methylmalonic acid in blood and urine [11]. MMA is the most prevalent organic acidemia in children [21], and affected individuals often suffer from multi-organ damage, with potentially life-threatening consequences [28]. Despite advances in medical care, particularly the implementation of newborn screening, these benefits are mostly seen in short-term outcomes. However, over the course of the disease, recurrent episodes of metabolic acidosis and hyperammonemia remain persistent challenges [40]. Survivors often endure a range of chronic complications, including growth retardation, kidney failure, neurological dysfunction, and cardiomyopathy, among others [14, 16, 20, 40]. These complications frequently lead to early mortality, increased hospitalization, and a reduced quality of life.
The guidelines for the diagnosis and management of PA and MMA have recommended dietary and nutritional modifications aimed at reducing the frequency and duration of metabolic acidosis and hyperammonemic episodes [4]. Dietary management has become a core, lifelong therapy for MMA patients [33], involving the restriction of natural protein intake alongside supplementation with precursor-free medical foods. This approach aims to minimize the accumulation of toxic metabolites while ensuring adequate intake of essential amino acids, thereby promoting nutritional balance, metabolic stability, and optimal growth [1, 4, 33]. Studies have demonstrated that non-adherence to dietary recommendations could result in compromised therapeutic efficacy, prolonged hospitalizations, and increased burden for both patients and caregivers. In severe cases, non-compliance can accelerate disease progression and even result in death [6, 15]. In particular, unrestricted protein intake among MMA patients is a well-documented trigger for metabolic crises, placing non-compliant individuals at significantly higher risk of severe, potentially fatal complications [4]. Therefore, strict adherence to dietary treatments is crucial for managing MMA effectively.
However, achieving consistent compliance with this specialized dietary therapy remains a significant challenge, particularly for children. While multidisciplinary teams—including healthcare providers, dietitians, genetic counselors, and pharmacists—play a crucial role in integrating dietary management into the overall treatment strategy, their efforts are often hindered by persistent barriers. These teams are responsible for designing individualized dietary modifications, conducting regular check-ups, and providing ongoing health education, and they also implement crisis prevention protocols and coordinate referrals to specialists to manage the condition more holistically [11, 12, 37]. Despite these efforts, dietary protein restrictions pose particular difficulties. Family caregivers, particularly those major managing the care of children with MMA, are required to meticulously plan and adjust dietary intake based on medical advice and frequent hospital test results. Since this treatment is typically applied at home, family caregivers encounter difficulties in adhering to the prescribed regimen without direct professional supervision. Furthermore, medical foods prescribed for these patients often have poor palatability, leading to resistance, especially in children, who may experience symptoms such as vomiting, lethargy, and poor feeding [31]. These barriers significantly impact treatment compliance. Moreover, the high cost of these foods adds to the financial burden, further compounding issues of non-compliance. Despite continuous support and follow-up from healthcare teams, previous interventions have demonstrated limited success in fully addressing these compliance challenges.
The World Health Organization (WHO) describes treatment compliance as a complex dynamic process of individual behavior influenced by various factors, including social, economic, therapy-related, patient-related, situational, and health system-related elements [5]. These factors can be categorized as either internal or external to the patient. Undoubtedly, patients and their caregivers are the key part and final arbiters of a range of factors, and in the end, it is they who either do or do not follow the doctor’s advice and what is prescribed [30]. In addition, external factors such as improving taste or reducing medical foods prices to improve dietary treatment compliance cannot easily be modified in the short term. Thus, focusing on the internal factors is what’s most tangible and easiest to improve, which is also the most-studied area in clinical practice [30]. According to health belief model (HBM), the more patients and their caregivers are aware of their conditions and the significance of treatment, the more they can exert their subjective initiative related to health behavior, and the higher their compliance [32]. Thus, patients’ and their caregivers’ perception and correct understanding of the disease-related information is among one of the most important internal factors.
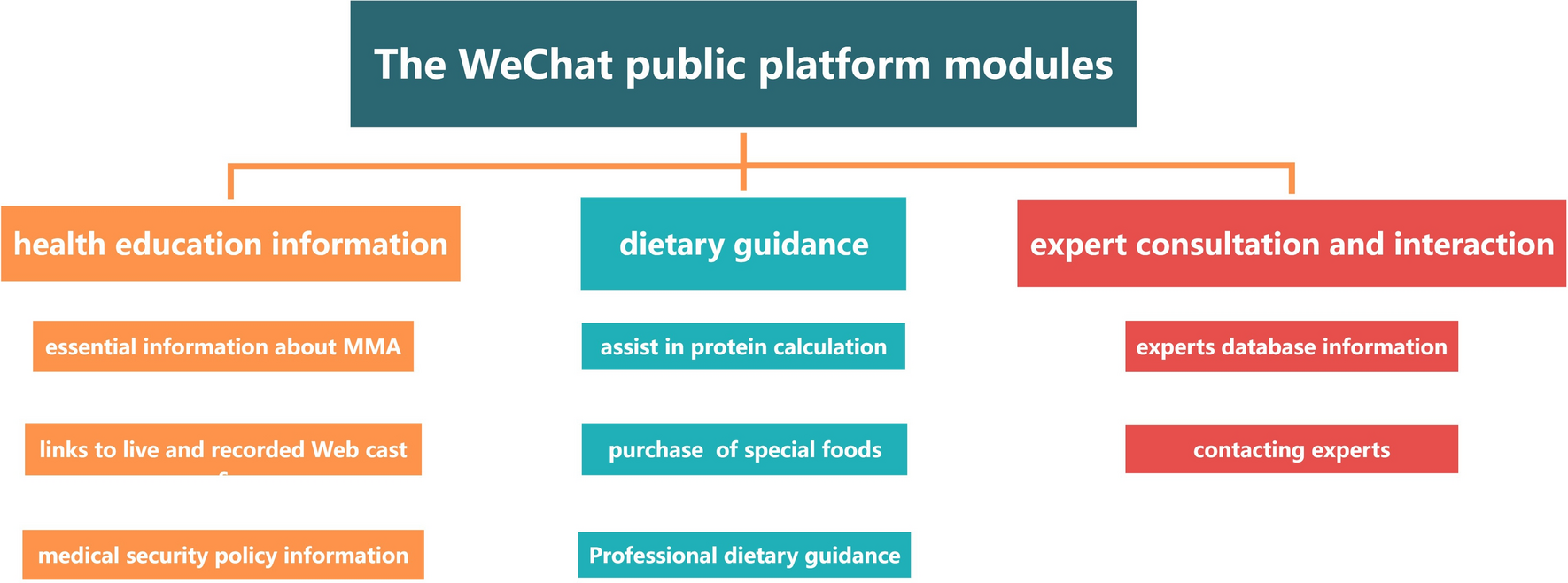
Recently, social media platforms have become a growingly popular source for health information and dissemination [39]. WeChat, one of the world’s largest mobile applications with 1.1 billion monthly active users, has gradually emerged as the most popular platform for health education in nursing management in China [38]. Studies have shown that WeChat-based health education programs can effectively improve patients’ health behavior, self-management ability, and treatment compliance in some diseases with similar situations in low treatment compliance, for example, in patients with cancer [17, 24] and chronic illness [10, 18]. Given these, WeChat-based health education is also likely to present new opportunities to facilitate dietary treatment compliance among children with MMA. Despite this promise, there remains a scarcity of research specifically investigating the role of WeChat-based health education in improving dietary treatment compliance in this patient population. To our knowledge, this research is one of the first attempts to use a WeChat-based platform to intervene in dietary compliance among children with MMA. The primary aim of our study was to fill this gap by exploring the potential effect of WeChat-based health education in supporting long-term dietary compliance among children with MMA. Through this research, we aim to identify effective strategies and interventions that could promote sustained adherence to dietary treatments, ultimately improving patient outcomes.








Comments (0)