
Remember me


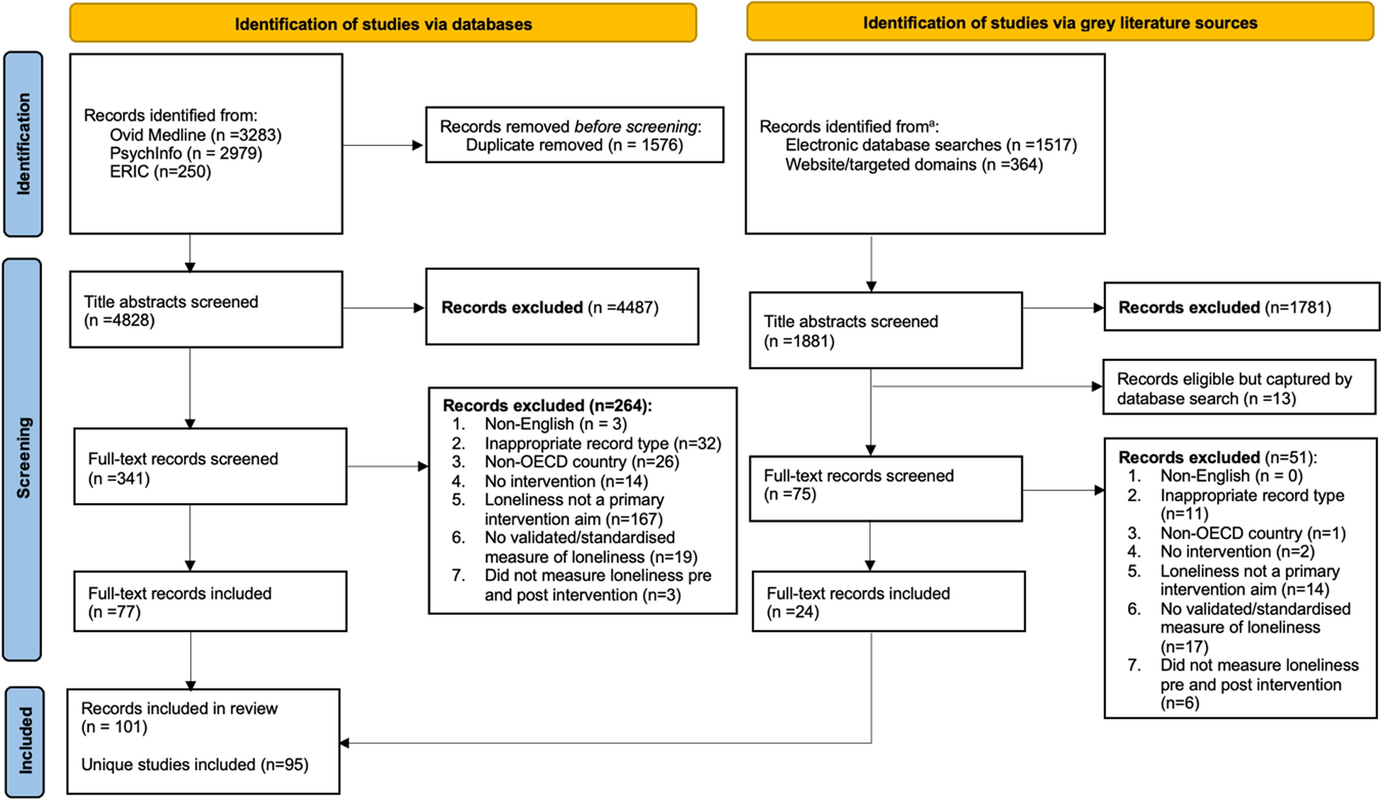
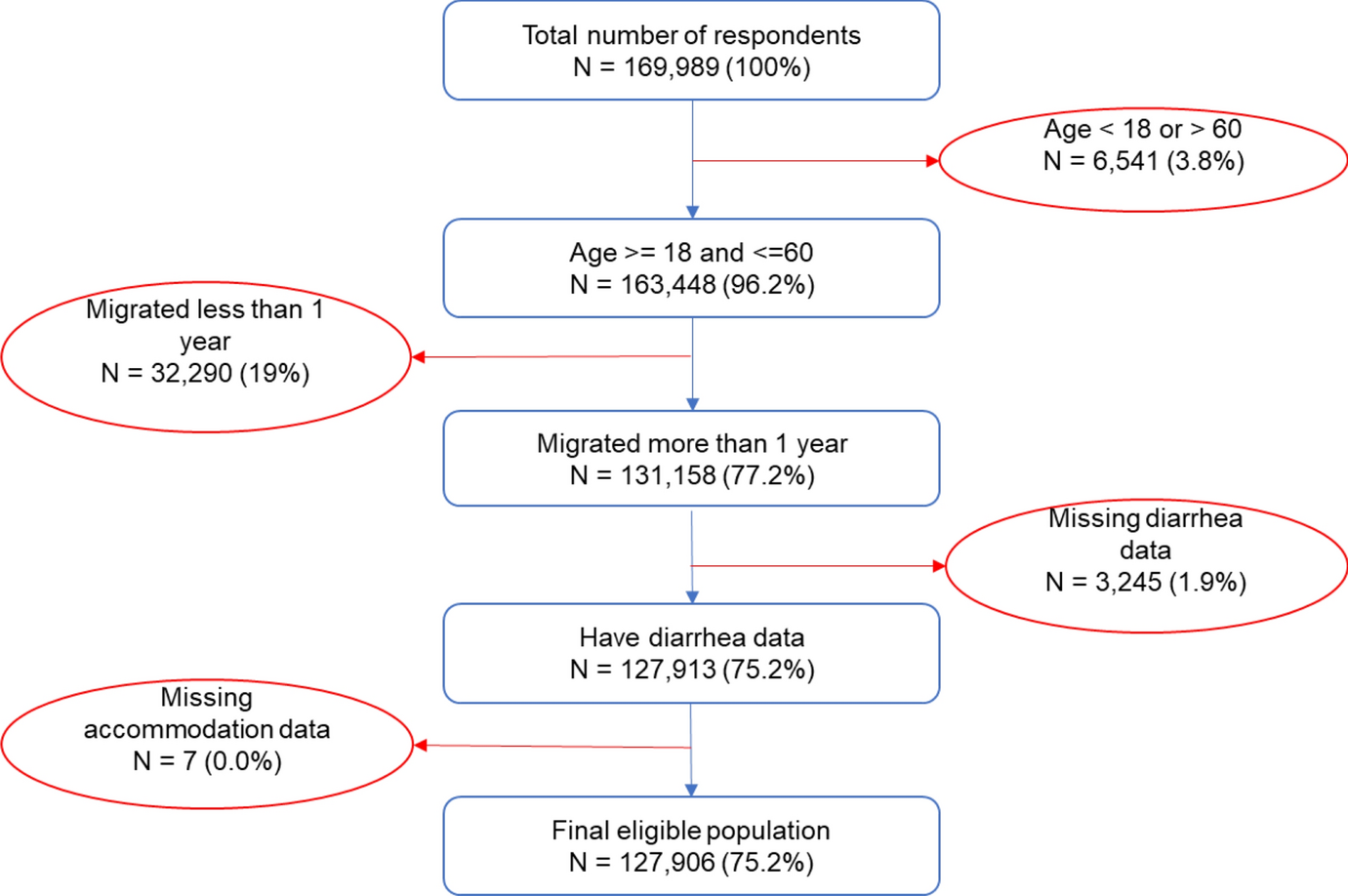

We identified 367 studies for the initial review of titles and abstracts, and from that review, we selected 40 studies for a full-text review. We included 24 studies in the final data synthesis and extracted policy-relevant information from each of the studies [20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43]. We excluded 16 papers due to a lack of topical relevance to the research question or poor methodological quality (see Fig. 1 for a flow chart illustrating the study inclusion and exclusion criteria).
Fig. 1
Inclusion/exclusion criteria flow chart
The 24 studies encompassed cities from 12 different countries: 6 studies from Europe (Germany, France, Portugal, Spain, Italy, Norway), 10 from North America (the United States and Canada), 1 from Euro-Asia (Turkey), 5 from Asia (Singapore and India), and 2 from Africa (South Africa and Kenya). Based on this breakdown, the study was primarily focused on North American and European urban areas. Within Asia, most studies focused on Indian urban areas. Notably, most studies did not differentiate between subgroups of migrants.
We identified additional differences in the contextual factors that impacted the health and health outcomes of COVID-19 urban migrants. For example, local COVID-19 severity/incidence was heightened in European countries such as Italy, Spain, and France as well as the United States (US), which were early epicenters of the pandemic in April 2020 [20, 21]. Similarly, the local COVID-19 policy context in the various countries had a tremendous impact on migrants. This could be seen when comparing policies in social welfare states vs dependence on unemployment/CARES Act in the US [22, 23].
Underlying structural inequitiesMigrant communities are more likely to have a lower socioeconomic status than their host community, thus exacerbating their vulnerability to the COVID-19 pandemic [24]. Several studies confirmed this trend in large urban areas [24,25,26]. Migrants experienced disproportionate losses in employment, financial stability, and access to and utilization of public and healthcare services [25,26,27]. In Istanbul, migrants were financially more impaired than their rural counterparts [28]. Similarly, early in the pandemic in cities in the US, migrants who were unable to work from home reported disproportionate financial insecurities. This directly affected migrants as well as their families in origin countries due to loss of remittances [29]. Following new COVID-19 policies designating “essential worker” occupations, many migrants were unable to stay home from work, placing them at an increased risk of COVID-19 [26, 28]. Underlying socioeconomic inequities were further exacerbated by limited access to community and healthcare services and the exclusion of most migrants—particularly undocumented migrants—from safety nets and relief funds [25, 26]. In some countries, for example in Istanbul (Turkey), urban migrants were excluded from relief funds, whereas rural migrants were not, causing an urban–rural exodus [28]. Furthermore, xenophobia and discrimination against migrant communities during the pandemic contributed to unequal job opportunities and underutilized services, as demonstrated by case studies from Durban (South Africa), and New York City (US) [25, 30].
The disproportionate impact of COVID-19 on migrants in large urban areas could also be attributed to language barriers, cultural discrepancies, and higher rates of unauthorized employment compared to rural areas, which was particularly pronounced among undocumented migrants. Language barriers were especially a source of health inequities during the COVID-19 pandemic as they could hinder public health messaging and communication with the healthcare workforce [32]. In the United States, people whose preferred language was not English were more likely to test positive for COVID-19 [33]. In Canada, people with language barriers had limited access to information and services which might have increased their exposure to the virus and hospitalization, while a large percentage of them did not have access to interpreters after hospitalization [34]. Migrant-serving organizations in New York City advocated for the need to provide language translation and interpretation assistance, as multilingual health information was essential in the context of the COVID-19 pandemic to improve community knowledge and prevention [35, 36].
We determined other factors that could also be responsible for further marginalizing migrants and exacerbating existing vulnerabilities. For example, elderly, disabled migrants faced more challenges compared to young, healthy migrants [37]. This emphasizes the role of the intersectionality of the different social categories for individuals and communities on health inequities. We found that underlying socioeconomic and structural inequities were pronounced in large urban areas and impacted migrants disproportionately. Efforts to address these underlying inequities may help mitigate the impact of the health crisis on migrants and should be considered in policy solutions.
Implementation of COVID-19 policies and proceduresVarious studies demonstrated the impact of policies and procedures as both exacerbating and mitigating factors vis-a-vis COVID-19 and migrant groups in large urban areas. Inaction from city and state governments led to migrants’ exclusion from economic relief programs, such as stimulus money, unemployment benefits, or salary continuation after the closure of businesses [25, 38]. This was especially pronounced for undocumented and temporary migrants and was further exacerbated by bureaucratic and language barriers and the fear of “becoming visible” to immigration authorities [25, 29]. In the US, the Immigration and Customs Enforcement agency failed to contain the spread of COVID-19 within detention centers in Newark, New Jersey [39]. Both the exclusion of and failure to protect migrant communities highlighted how government actions (or lack thereof) can exacerbate the impact of COVID-19 among migrant communities in large urban areas [39].
In addition, anti-immigration and exclusionary policies deterred migrants from leaving their host country, limiting both circular and return migration. Policies like the Public Charge Rule in the US led to increased fear of deportation [40]. According to this rule, immigration rights could be denied if overuse of public benefits is suspected and thus an immigrant becomes a “public charge.” Public benefits include Medicaid, rental assistance, and the Supplemental Nutrition Assistance Program, which are critical programs for marginalized, low-income communities [40]. While the rule targeted immigrants prior to their immigration, some migrants who resided in the US avoided utilizing such public benefits or services due to fear of becoming “visible” and risking a change in immigration status or deportation [38, 40, 41].
Alternatively, e-governance and technology showed potential for increasing access to public services [30, 31]. E-governance is defined as the utilization of technology by national, state, or municipal government offices to enhance access to their services and/or improve communication between government structures and constituents [30]. However, e-governance and transferring services to the online sphere may still pose unique difficulties for migrant communities. Without personal contact or translation services, language barriers may be amplified [7]. In addition, crowded housing may pose privacy issues where migrants are not comfortable sharing personal information through teleservices [42, 43]. A lack of access to the internet and/or other communication devices also disproportionately affected communities who had fewer resources available, such as migrant communities [42]. To maximize the mitigating effects of e-governance and teleservices, barriers to these services for migrant communities must be addressed [43, 44].
Urban designEvidence suggests that urban design impacted the spread of COVID-19 in large urban areas. Some studies highlighted the negative aspects of residential segregation in large urban areas, which is associated with precarious living conditions [45,46,47]. The National Bureau of Economic Research defines housing precarity as a situation in which the resident may be at risk of eviction [48]. The main reason for precarious housing during the pandemic was employment insecurity and the inability to pay rent [48, 49]. Higher rates of unemployment during the COVID-19 pandemic exacerbated precarious living conditions [48]. As a result, many migrants felt obliged to keep working in often overcrowded or high-risk occupations to prevent evictions or utility disconnections [48].
High-density living arrangements in remote or outlying areas of cities also led to greater spread of COVID-19 and a greater impact on migrant communities living there [46, 47]. An example from Singapore showed that migrants often traveled great distances to other parts of the city for job opportunities and essential services, such as grocery stores and medical resources [47]. However, a high utilization of public transportation during the COVID-19 pandemic exposed migrants disproportionately to the virus, especially when other means of transportation such as walking or biking were not feasible [46, 47]. Hence, during emergency situations, it needs to be ensured that essential services are not only available in city centers, but in remote or outlying areas as well [47].
While these are crucial findings, the literature on how urban design exacerbated the COVID-19 impact for urban migrants has been scarce. To our knowledge, very few or no mitigating effects of the urban design on COVID-19 impacts for migrants have been documented.
Engagement of Civil-Society OrganizationsSeveral studies identified the engagement of CSOs as an important mitigating factor on the impact of COVID-19 on migrant groups in large urban areas. In many cities, CSOs filled governmental and institutional gaps that excluded migrants by providing food, necessities, childcare, translation services, COVID-19-related information, and cultural mediation [42, 44, 50, 51].
For example, in Germany, Chinese Heritage Schools adapted to include more childcare services to cater toward the specific pandemic-related needs of their community [50]. Cultural mediation also included utilizing health care navigators to connect migrants with health care providers, services, or health-related information [52]. This is particularly important during a public health crisis such as COVID-19 to combat misinformation, overcome language barriers, and increase access to medical care [42]. In practice, health care navigators are often migrants themselves or have extensive experience with migrants’ barriers and needs [52]. By providing information in migrants’ native language, information asymmetry can be reduced. In addition, health care navigators were able to accompany migrants to health care services such as COVID-19 testing and treatment [52]. CSOs also created and managed extensive networks of volunteers, translators, and health and law professionals to improve access to care and services [40]. For example, in the US, CSOs provided information about eligibility for government benefits and combated misinformation regarding the Public Charge Rule [40].
CSOs and the provision of COVID-19 technologiesIn some cities, CSOs used technology to move mental health consultations online and provide information through video conferencing [42, 43]. However, this mitigating effect was hindered by a lack of access to devices or the internet or a lack of understanding of how certain software should be used [43]. CSOs can play an important part here as well. By working with migrant communities, introductory sessions can be hosted to introduce technology and instructions can be distributed in various languages [43]. In addition, some CSOs placed value on including other migrant family members in the process of teaching technology and alternative services to enable migrants to access these services [43].
As laid out, CSOs played a significant role in mitigating COVID-19 impacts for migrant communities. However, these mitigating effects are contingent on two factors: (1) a trust relationship between CSOs, volunteers, and communities in need, and (2) systematic organization of efforts [44, 53]. Municipal governments should therefore recognize and support the efforts of CSOs to enable more targeted, systematic organization of assistance [44].
Comments (0)