Biomodels of vital structures of the human body are widely used in research. Analysing these biomodels by finite elements reduces time and cost compared to other studies. It provides predictions that can aid in choosing the best technique for each mechanical and physiological requirement. In addition, it does not involve ethical issues or the need for clinical intervention [4, 9, 12, 19, 20]. The validation of mandibular biomodels and their finite element analysis has already been performed, showing a correlation coefficient of 0.992 [9].
In Puricelli osteotomy, the increase in the area of the proximal segment and the consequent decrease in the lever arm applied to the mandible provide lower values of stress and displacements. The magnitude of the displacements indicates mandible stability; thus, lower values indicate greater stability of the bone segments. It is suggested that, in vivo, there is greater stability, with a decrease in the lever arm, resulting in better repair, decreased displacement due to muscle activity, and, consequently, a reduction in the period of elastic intermaxillary immobilisation [6, 12].
This study used FEA to compare the Obwegeser–Dal Pont and Puricelli techniques for mandibular advancements. A previous study evaluating mandibular osteotomies without segment displacement showed that the Puricelli technique results in lower stress and displacement values compared to the classical technique of Obwegeser–Dal Pont [12].
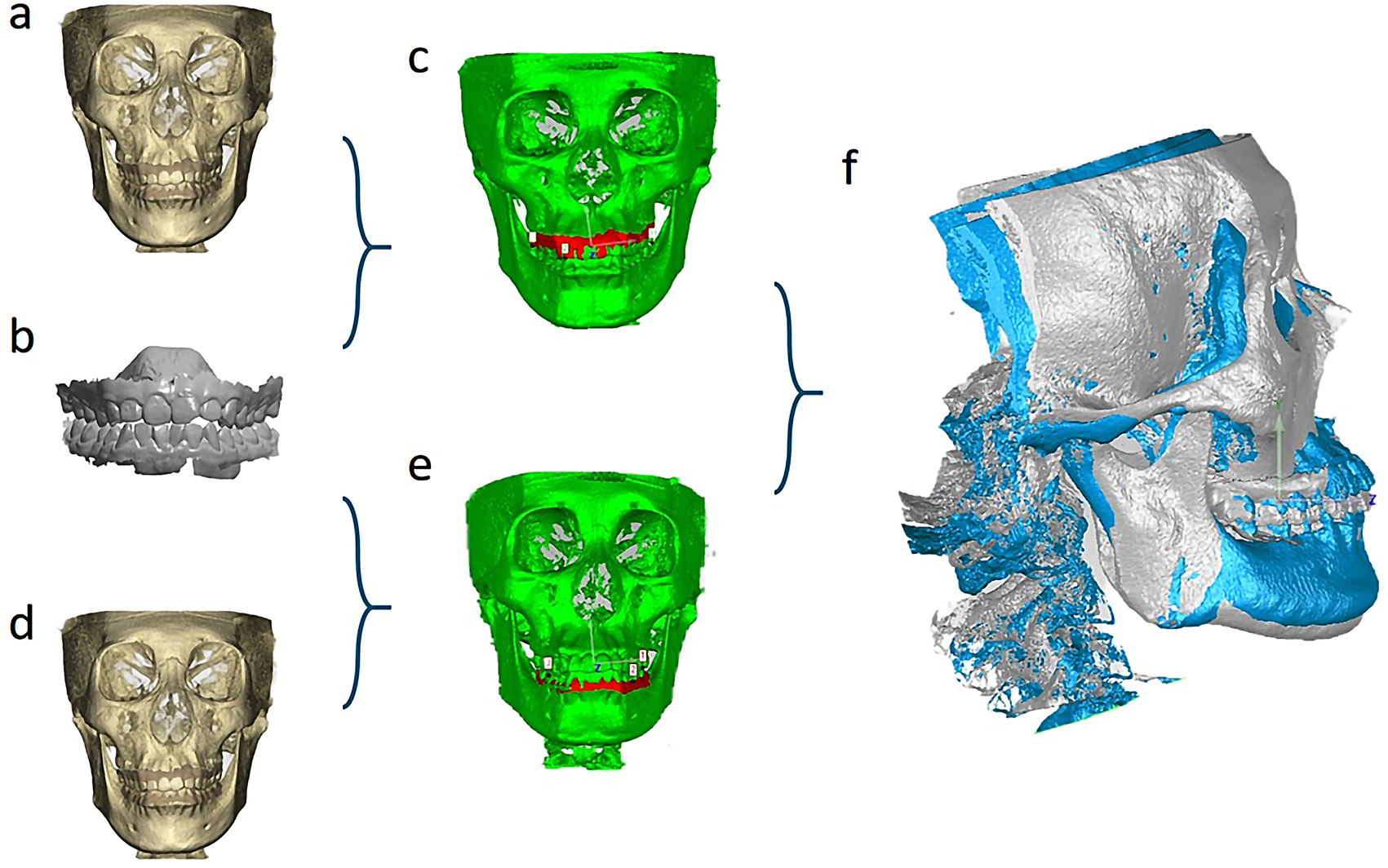
The present study was based on the geometric model published by Amorim Vasco et al. (2016) [10], and the properties of the materials were based on the studies by Puricelli et al. (2007) and Chang et al. (2019) [12, 13]. A virtual model of the hemimandible was used for a comparative analysis, with a unitary force (1 N) applied in the anterior region of the left hemimandible and stabilisation performed in the left mandibular condyle region [21]. Since the FEA was based on a linear model, these qualitative results are valid for other loads. As it was not the object of this study, the effect of contact stresses at the interface between the plate and the mandible was not evaluated [12].
FEA of mandibular stability in mandibular advancements ranging from 3 mm to 10 mm have been reported but not associated with Puricelli’s mandibular osteotomy [14,15,16, 21,22,23,24,25]. Mandibular advancements of 10 mm or more are considered ‘major advancements’ and present a higher tendency for relapse [17, 26, 27].
In this study, the 10 mm mandibular advancement is justified given the increasing indication of BSSO for treating patients with large skeletal discrepancies and obstructive sleep apnea-hypopnea syndrome (OSAHS). Great mandibular advancements increase the pharyngeal airspace with distension of the velopharyngeal and suprahyoid muscles, benefiting patients with OSAHS [28] and increasing the effectiveness of surgical treatments [29].
The Puricelli technique resulted in a 17.48% higher mandibular stress than the Obwegeser–Dal Pont approach. In the comparison of osteotomy methods, the point of greatest stress is distant from the area of fragility resulting from vertical osteotomy and the region of fixation of the osteosynthesis media (plates and screws), thus suggesting greater stability after Puricelli osteotomy. In the evaluation of the hemimandible displacement, it was observed that Obwegeser–Dal Pont osteotomy resulted in a displacement 40.32% greater than the Puricelli technique.
The system of third-class levers can be applied in interpreting the stress and displacement evaluation [4, 30]. The temporomandibular joint represents the fulcrum, and the application of force to the anterior region of the hemimandible represents a force vector. In comparing 10 mm mandibular advancements, the more anterior the vertical line of the mandibular osteotomy is performed, the greater the distance from the high-stress area and the smaller the displacement. The anteriorisation of the vertical osteotomy of the mandible ensures greater stability [18], unlike the vertical osteotomy in the classic Obwegeser–Dal Pont technique, which is performed near the region of greater mandibular fragility (mandibular angle) [31].
Considering the area of overlap between the proximal and distal segments of the mandible, the results of the GTP10 group show an area 33.13% larger than the GTOD10 group. The maximisation of the overlapping area indicates the greatest possibility of contact and is related to the surgical technique employed [29]. In mandibular osteotomies, there is no treatment on the bone surfaces and the gap to guide bone neoformation. The bone repair depends on the space between the osteotomy lines, anatomical location, mechanical/muscular forces at this site, and the patient’s age and systemic condition [32,33,34]. The larger area of overlap between the osteotomised segments and the anteriorisation of the vertical line of osteotomy, observed in Puricelli’s mandibular osteotomy, results in an increase in the area of medullary exposure and in the organisation of a clot, consequently favouring bone neoformation. The larger extension of the overlapping surface shows a significant association with the decrease in the mean or maximum stress value [35]. In addition, the smaller the contact surface, the greater the risk of postoperative fracture [29].
The condition of greater sliding of the segment corresponding to the body of the mandible, offered by the Puricelli technique, allows for an average 18 mm increase in the proposal of advancement. Even in the acute traction and stretching of the inserted muscles and the mucosa, vascularisation is not affected when properly handled.





Comments (0)