
Remember me





Design. To accomplish the first objective of implementing the opioid risk metric thresholds into the PDMP platform and adapting the platform for intervention delivery, our investigative team is collaborating with leadership from the PDMP partner organization as well as the chain pharmacy organization to incorporate the risk metric thresholds and adapt the PDMP platform for intervention delivery (in the same chain pharmacy corporation mentioned above from CTN-0093). This objective is specifically following the Guideline Implementation with Decision Support (GUIDES) Checklist [32]. The development of GUIDES was originally motivated by the significant potential of decision support tools for implementation of evidence-based practice, yet there have been limited outcomes in previous research literature in terms of use, sustainability, and patient impact [33,34,35]. Given the complexity of clinical decision support systems, GUIDES was developed by an expert panel to provide structured steps to follow for the development, implementation, and monitoring of decision support tools [32]. GUIDES has four steps, which include: [1] examining the context [2], organizing content [3], ensuring high quality user access, and [4] implementing the ORRCDS tool (see Table 1). Note, steps one and two were targeted for completion within the first ~ four months of the project; step three was targeted for completion within the first ~ 10 months of the project, and step four was targeted for completion within the first ~ 18 months of the project.
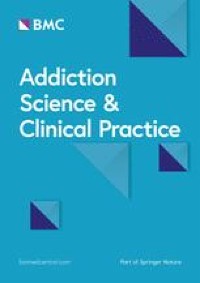
The examining the context step of GUIDES involved working with the partnering chain pharmacy to assess existing clinical workflow. To do this, we collaborated with compliance and clinical program development pharmacy corporate leaders who understand regulatory and clinical operations related to opioid dispensation to identify optimal opportunities for when the ORRCDS is triggered in workflow. This workflow assessment allowed tool planning to balance optimizing patient management while accommodating practice demands of pharmacists and technicians. Lastly, this step involved working with the PDMP partner as well as the pharmacy compliance and clinical program development leaders to determine actual workflow within the ORRCDS itself for staff use, see Fig. 1.
Fig. 1
ORRCDS tool flow chart. a Narcotic score. b This flow chart only applies to Rx opioid risk. Non-Rx opioid substance screening may be feasible under other circumstances. c WHO Alcohol, Smoking, and Substance Involvement Screening Test prescription opioid use risk assessment. d Pain, Enjoyment, General Activity. e Brief intervention for prescription misuse. f Brief intervention for treatment linkage. g Treatment. h Prescription Drug Monitoring Program
Table 1 GUIDE framework areas of outcome assessmentThe organizing content step of GUIDES involved our study investigators as well as pharmacy chain partners laying out all of the ORRCDS content. Briefly (see greater details in the intervention section below), ORRCDS will categorize patients into low, moderate, and high risk. Moderate- and high-risk status based on risk metric scores will be confirmed by a brief self-report assessment (i.e., the ASSIST prescription opioid risk subscale; [30, 31]. These measures were selected given their clinical utility while at the same time being able to accommodate the pharmacy locations and related demands in terms of brevity. False positive patients will be assessed for pain (i.e., the Pain, Enjoyment of Life and General Activity scale [PEG] [36]) and provided resources. Moderate risk patients will be provided with a brief motivational intervention to reduce opioid risk behaviors and given resources—including naloxone referral. High risk patients will be provided with a warm handoff to their primary care provider delivered in the style of a brief motivational intervention to discuss addiction and other treatment options. These patients will also be provided a naloxone referral for a kit to be mailed to them free of charge (see Fig. 1). The content for each risk level was created by developing scripts utilizing brief motivational intervention principles coupled with normative feedback.
The ensuring high quality user access step included adapting the existing PDMP platform in collaboration with PDMP and pharmacy partners to ensure screening, motivational intervention/feedback, naloxone recommendation, and warm handoff/treatment linkage tools are easy to use, well-delivered, and activate at optimal times. This has involved an iterative approach with the investigative team presenting ideas and designs for ORRCDS, incorporating those ideas and designs into mock-up slides, reviewing these slides with investigators and pharmacy/PDMP leaders, and then revising the mock-up slides based on feedback.
The final step is implementing the tool, which entails two parts. The first is actual tool implementation within the PDMP and pharmacy chain systems. ORRCDS implementation followed the pharmacy chain standard 3-phase approach: (1) pilot site initiation over 1 month; (2) receive feedback from staff/make needed adjustments; and (3) full study testing thereafter. The second part established a training module with the chain pharmacy required for pharmacy staff before site initiation of the intervention (see details below).
Measurement and analysis. Objective 1 will be assessed using the GUIDES evaluation framework. This framework includes 4-items per above specified domains, each with a 7-point Likert scale for scoring [32]. This tool will be administered to study stakeholders including investigators, corporate leaders from pharmacy sites and PDMP partners, and a National Institute on Drug Abuse Scientific Officer (assigned to the project by virtue of the cooperative agreement funding mechanism). We will also utilize the System Usability Scale, a brief 10 item measure of perceived computer-based program usability [37, 38], to assess the yes/no go-live readiness of ORRCDS. This assessment will be administered to pilot pharmacy site staff who utilize the tool.
Frequencies, percentages, and measures of central tendency will be employed to assess results from the GUIDES responses. Specifically, each of the above Likert scale items will be described using mean and standard deviation as well as median and interquartile range. For the supporting items, which are yes/no responses (not shown herein), we will calculate frequencies and percentages to characterize responses to these items. For the System Usability Scale, we will summarize the overall score. A score of 68 or higher is considered the cut off for yes/no usability [39, 40]. Having the subjective GUIDES assessment as well as the objective System Usability Scale provides rich insights for the investigative team into the readiness of ORRCDS and avenues needed for improvement before full trial launch.
Objective 2: Testing the ORRCDSDesign. To accomplish the second objective of this study of assessing the impact of the ORRCDS tool on patient opioid risk, our study team will conduct a type-1 implementation mixed methods study using a 2-arm parallel group clustered randomized design. This design clusters patients within pharmacy sites, randomized on a 1-to-1 basis to the ORRCDS vs. usual care. We chose the cluster design given its advantages over patient-level randomization and the length of time required by stepped-wedge designs. Regarding patient level randomization, given the real world application of this tool, training staff to deliver the intervention to only some patients within sites and not others would create a greater risk for condition contamination compared to randomizing by site. The cluster design will reduce the possibility of patients being exposed to both conditions, thus preventing contamination. Regarding length of time, a stepped-wedge design that would attempt intervention rollout in 80 busy pharmacy sites would require a prohibitive amount of time for site intervention delivery initiation, intervention utilization, and follow up.
The randomization will be stratified by zip code poverty level and total pharmacy volume of medication dispensed. Stratification by dispensing volume will ensure an even distribution of higher vs. lower volume stores in each condition—given that high volume sites may be more likely to not intervene with each patient given more intense workload. Advantages of site- vs. patient-level randomization include strengthened internal validity from mitigation of potential condition contamination as well as lower costs—given the number of sites and patients involved herein. ORRCDS will be evaluated within two divisions of a pharmacy chain (n = 40 intervention pharmacies/n = 40 usual care pharmacies) in the state of Ohio. This design includes a 6-month enrollment phase and a 6-month follow up observation phase (see Fig. 2).
Fig. 2
Study design. * Opioid risk reduction clinical decision support
Study population. Data from patients within pharmacy clusters will be utilized for analysis. Those patients prescribed an opioid medication, seeking opioid prescription dispensation in a study pharmacy, ≥ 18 years of age, and who have an opioid risk metric of moderate or higher will be included in the study cohort. Those solely receiving buprenorphine formulations for opioid use disorder treatment, without an additional dispensation of a pain medication during the study intervention exposure period or those that received the majority (more than 50%) of their opioid medication dispensations (other than buprenorphine) from non-study pharmacies will be excluded. These data will be obtained from the PDMP database for the state based on a waiver of consent approval from the University of Utah Institional Review Board.
Interventions, training, and supervision. Discussed briefly above, the ORRCDS condition involves ORRCDS alerting the pharmacist during the drug utilization review process that a potentially at-risk patient has an opioid medication in queue for pickup; these alerts are based on the previously identified thresholds from the PharmScreen preliminary study [10]. Patients identified as moderate or high risk would receive confirmatory opioid misuse screening. Those identified as low-risk on confirmatory screening will receive auxiliary pain screening on the PEG [36]. Patients reporting moderate/high pain with low opioid risk will receive non-opioid pain management information/education [41]; such education may increase the utilization of non-opioid pain management strategies [42].
Patients with moderate risk on confirmatory opioid misuse screening will receive a brief motivational intervention incorporating normative feedback that targets behaviors associated with opioid misuse (e.g., early refills of opioid medication, seeking multiple opioid prescriptions) coupled with naloxone recommendation and referral. The ORRCDS tool is designed to assist pharmacists in systematically assessing and intervening in cases of risky prescription opioid use and management. This tool will guide the pharmacist through an evaluation of the patient’s risk factors and potential barriers to change, employing motivational interviewing techniques to engage the patient in exploring safety driven behavior change. The risk factors targeted for intervention include, as listed above, opioid dosages, overlapping benzodiazepines and opioid medications, overlapping opioid medications, and numbers of prescribers and pharmacies utilized by patients. Based on the assessed risk level, the tool facilitates a warm handoff to primary care and encourages the patient and primary care provider to discuss a connection to specialized treatment when possibly needed. This approach aims to effectively address opioid misuse while fostering patient-centered care.
In at least four separate clinical trials (N = 32, N = 62, N = 126, N = 204 [9, 43,44,45]) with patients receiving brief motivational interventions to reduce opioid medication misuse/misuse behaviors, study results showed significant improvements [9, 43,44,45]. In either scenario of moderate or high risk, the pharmacist’s goal is to assist the patients in making health behavior changes to reduce risk—the goal is not to deny or take away access to opioid medication treatment, which could result in detrimental unintended consequences [46,47,48].
Those with confirmed high risk will receive a warm handoff delivered in the style of a brief motivational intervention to connect patients by phone to their primary care provider to discuss substance use treatment or other treatment needs (such as pain management). These patients likewise will receive a naloxone referral. A rich literature shows warm handoff is an evidence-based method for connecting individuals with substance use needs to treatment [49,50,51,52,53]. Patients with elevated risk will receive up to 2 intervention sessions over the course of up to 2 dispensation encounters with pharmacists—interventions will be similar each session if risk status does not change between encounters. The maximum duration for an opioid prescription in Ohio is 90 days.
ORRCDS training will involve pharmacists at the intervention pharmacy sites being emailed brief reading materials regarding the foundational work of this project. Next, a series of web-based, pre-recorded trainings that instruct pharmacists on using the tool will be made available via an electronic education platform. Pharmacists will be required to view the videos to familiarize themselves with the required steps of the intervention. The prereading and recorded videos each last approximately one hour for a total of two hours. Post tests will be administered in the education platform to ensure material comprehension and retention. Training completion/ attendance will be captured by the training platform.
The study team will also provide monthly supervision sessions during the 6-month intervention period. All intervention site pharmacists will be required to attend at least three of these zoom/telephone sessions to receive booster training from study staff and engage in question-and-answer discussions. Sessions will include didactic material, session examples, and question and answer periods. These supervision sessions will last approximately 30 min and attendance will be captured by study staff leading these sessions.
Intervention delivery performance monitoring will take place weekly by the PDMP vendor providing numbers regarding how many interventions were delivered at unique pharmacies along with the total number of patients in that week who received opioid medications. This will allow the study team to monitor total intervention opportunities and compare those to the actual number delivered and to allow the study investigators to provide site feedback and encouragement in the utilization of the tool.
For the usual care condition, pharmacists are required to perform a universal PDMP review before initial dispensations [54]. Pharmacists are also required to offer brief counseling (e.g., unstandardized information about medication safety) for new/modified prescription therapies [55]. Pharmacists are trained and monitored (via dispensing record system alert) for these requirements by the chain pharmacy partner.
Outcomes and data collection. Study data collection will follow the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) implementation science evaluation framework. Table 2 shows the specific indicators that will be employed in this study, ordered by primary/secondary outcomes [56]. Given the type-1 focus of this study, the primary efficacy outcome will be assessing changes across time for patients’ opioid risk metric level from high to moderate risk or moderate to low risk, see power calculation below. Mentioned above, this metric was validated in CTN-0093, using the WHO ASSIST [10]. Secondary efficacy outcomes will include possible improvements in measures of opioid utilization over time, such as changes in performance on opioid safety measures developed by the Pharmacy Quality Alliance including high opioid dose (greater than or equal to 90 morphine milligram equivalents over 90 days) and overlapping benzodiazepine use (see Table 2 [57,58,59]).
Sample size and power. We anticipate that ~ 6,600 (based on CTN-0093 pharmacy site estimates) moderate/high-risk patients (evaluated by the opioid risk metric) will be enrolled during the 6-month enrollment phase across the 80 pharmacies. The power calculation is presented for multiple scenarios with different assumptions of intraclass correlation (ICC) and effect size (Table 3). The proposed sample size will provide 96.3% power with 2-sided \(\:\)= 0.05 to detect a 3% or greater difference in responder rate between the intervention arm and control arm. Responders are defined as patients with moderate-risk at baseline who reduce to low-risk or those with high-risk at baseline who reduce to moderate or low-risk at 180 days post last intervention. Risk categories are defined by the thresholds identified in CTN-0093, mentioned above [10]. The power consideration assumes an ICC of 0.05, typical for clustered randomized trials of patient’s outcomes [60, 61]. Importantly, the numbers of pharmacies chosen in this study approximates that of a division within the pharmacy chain. Thus, the results herein will have a real-world reference size within the chain pharmacy corporation.
Table 2 Reach, effectiveness, adoption, implementation, and maintenance implementation science evaluation framework construct chartTable 3 Power calculation with different assumptions for intra class correlation and effective sizeAnalysis plan. The primary efficacy endpoint is the responder rate at 180 days post final intervention. We will fit a generalized linear mixed model to relate the primary outcome (i.e., responder status defined based on opioid risk metric) by treatment arm, controlling for baseline covariates including but not limited to the stratification factors, baseline risk level assessment, and other relevant/available patient characteristics, including patient age, sex, insurance status, and location using pharmacy zip code. To model the dichotomous response variable, we will employ the binary distribution with logit link. The random intercept and the unstructured variance covariance matrix will be used to account for within pharmacy correlation. If the model fails to converge, the compound symmetry structured variance covariance matrix will be used.
Objective 3: Assessment of long-term sustainability and viabilityDesign and target population. To accomplish the third study objective of assessing ORRCDS’s sustainability and viability for broader adoption and dissemination within large-scale pharmacy and corporate environments, our study team will execute cross-sectional qualitative interviews with pharmacists from the chain partner as well as non-partner pharmacists (n = 15), leaders from the chain pharmacy partner (n = 15), and leaders from the PDMP company (n = 15). Participants will be identified by referral from the pharmacy and PDMP partners as well as through outreach to professional licensing lists of pharmacists in the state of Ohio. Interviews will be designed to explore barriers and facilitators of long-term adoption and sustainability of the implemented tool within the pharmacy and PDMP practice and corporate environments. Interviewees will be selected using a purposive sampling approach. To be included as a participant in this interview, individuals must be a licensed pharmacist, pharmacy leader, or leader within the PDMP company and believe they can provide insights and opinions regarding the long-term adoption and sustainability of the tool.
Interview guide. We will employ the Consolidated Framework for Implementation Research (CFIR) as the foundation for the qualitative interview portion of this study [62, 63], see Supplement 1. The CFIR is a multidimensional model consisting of standardized constructs for understanding and approaching objectives across the continuum of implementation science [64], ranging from pre-implementation activities to post-implementation outcome analyses [65,66,67]. The CFIR has an extensive literature base for formulating and implementing evidence-based interventions in real-world practice [64]. The CFIR has been applied across a number of programmatic areas, including health care delivery, health care processes redesign, quality improvement, health promotion, and disease management on topics such as mental health, obesity, and high blood pressure [64].
We will employ the CFIR interview guide for qualitative research to assess barriers to, and feasibility of: ORRCDS use in pharmacy settings, system-level adoption and implementation, and continued tool use [62]. Items will be selected by the research team in collaboration with the chain pharmacy leadership and in collaboration with PDMP partners. Interviews will also explore pharmacist perception of ORRCDS acceptability by patients. Examples of topic areas to be queried will include perceived feasibility of ORRCDS utilization within the retail pharmacy practice environment. Interviews will further explore what challenges exist that could impede adopting ORCCDS, i.e., getting the tool into practice within the broader partner pharmacy system or pharmacies outside the partner system. Interviews will also explore what characteristics, conditions, or outcomes need to be presented to pharmacists and corporate leaders that will ensure long term consistent use of ORRCDS.
Qualitative sample size. Previous research has demonstrated sample sizes of 20 individuals are sufficient to achieve thematic saturation between the researcher and participants, which will generate rich data for elucidating complex relationships [68]. Previous research has also demonstrated samples of approximately 12 interviews can reach saturation of findings [69]. Saturation has been defined as a point beyond which no significantly new information is being obtained. Lincoln and Guba’s framework [70] will be used to address and meet criteria for quality and rigor in this study and involve credibility, dependability, confirmability, and transferability [70].
Qualitative analyses. For the qualitative data, we will follow methods recommended by Braun and Clarke to capture associations between categories and extract and conceptualize themes [71]. We will independently review interview data and code inductively and deductively. Codes will be clustered based on their similarities into categories. Our team will meet multiple times to discuss the emergent themes [71]. Coded data will be described using frequencies and percentages.
Comments (0)