In this mechanistic analysis of the SUMMIT trial, we found that, compared with placebo, treatment with the long-acting glucose-dependent insulinotropic polypeptide receptor and glucagon-like peptide-1 receptor agonist tirzepatide reduced BP and estimates of circulatory volume expansion in patients with obesity-related HFpEF. These effects were observed early and were sustained with longer duration of treatment. Tirzepatide reduced systemic inflammation, but this effect was observed later than the hemodynamic effects. Tirzepatide resulted in an early trend to reduction in eGFR at 12 weeks, but this was followed by an improvement in eGFR compared with placebo with longer duration treatment, and reduction in microalbuminuria. Tirzepatide reduced myocardial injury compared with placebo, reflected by a significant decrease in troponin T, along with a reduction in NT-proBNP. Reductions in estimated BV with tirzepatide were correlated with decreases in systolic BP, reduction in UACR and improvements in both KCCQ-CSS score and 6MWD, suggesting that mitigation of circulatory volume expansion (or factors responsible for volume expansion) may play a central role in mediating the benefits of tirzepatide. Conversely, decreases in systemic inflammation with tirzepatide were correlated with reductions in cardiac injury with tirzepatide, along with a modest correlation with improvements in 6MWD. These findings provide new insights into the mechanisms by which tirzepatide leads to clinical improvement in HFpEF.
Obesity-related HFpEF is the most common phenotype of this disorder3,9, and its emergence is causally related to the growing burden of cardiovascular–kidney–metabolic disorders observed worldwide4. As compared with nonobese HFpEF, patients with obesity-related HFpEF display distinct pathophysiologic features, including greater volume expansion5,17, more severe inflammation6,7, increases in visceral and paracardiac adipose tissue5,15,18,19 and more severe myocardial injury15. Indeed, volume expansion, CKD and greater burden of hypertension best distinguish individuals from obesity-related HFpEF from age, sex and BMI-matched patients with obesity but no HF9. Collectively, these observations suggest that novel treatments that reduce circulatory volume–pressure overload (or its determinants), improve kidney function, reduce inflammation and mitigate cardiac injury may improve clinical status in people with obesity-related HFpEF.
In the SUMMIT trial, tirzepatide reduced the combined risk of cardiovascular death or worsening HF, and improved health status and exercise tolerance in patients with obesity-related HFpEF16. These results are consistent with findings observed in the STEP-HFpEF program, where the glucagon-like peptide receptor-1 agonist semaglutide was also shown to improve health status and exercise capacity20,21. The magnitude of improvements in health status and exercise tolerance with semaglutide were correlated with the degree of body weight reduction22, but the mechanisms underlying clinical improvement with incretins such as tirzepatide and semaglutide in patients with obesity-related HFpEF have remained unclear.
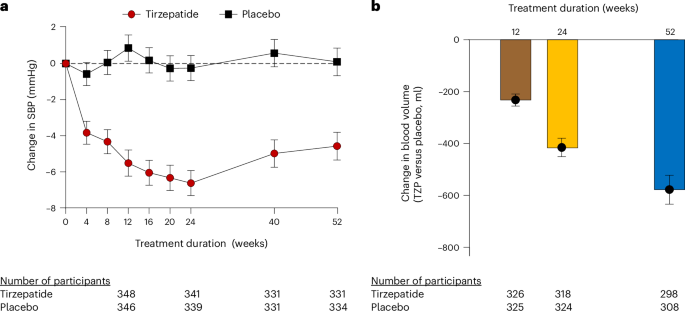
Here, we show that tirzepatide reduced circulatory volume expansion using estimates of BV and PV, an effect that was evident after just 12 weeks of treatment and that further increased at 24 and 52 weeks. It is noteworthy that adipocytes release factors that promote sodium retention and volume expansion, including leptin and aldosterone, and the reduction in adipocyte mass with tirzepatide may reduce these influences23. Volume expansion in obesity-related HFpEF exacerbates elevation in cardiac filling pressures that develop due to impairments in left ventricular distensibility3, and thus, reducing circulating volume may decrease cardiac filling pressures. This finding could partly explain the direct correlation observed between reductions in BV and improvements in KCCQ-CSS score and exercise capacity.
Tirzepatide also decreased systolic BP, an effect that was evident after just 4 weeks, and was also associated with reductions in estimated BV and PV. Effects on diastolic BP were not apparent, and thus, there was a significant reduction in pulse pressure. Pulse pressure is inversely correlated with arterial compliance, which is frequently impaired in patients with HFpEF, where increases in aortic stiffness contribute to elevation in cardiac filling pressures, especially during exercise24. Treatment with the sodium–glucose cotransporter 2 inhibitor dapagliflozin was recently shown to reduce aortic stiffness, systolic BP and pulse pressure during exercise after just 24 weeks, and these changes were correlated with reductions in left ventricular filling pressures25. The magnitude of improvement in arterial compliance with dapagliflozin was correlated with the magnitude of weight loss. Further study using more direct measures is indicated to determine whether tirzepatide also improves arterial compliance, which would be consistent with the effects on systolic and pulse pressure observed here.
Obesity can contribute to CKD through multiple mechanisms including volume expansion (leading to glomerular hyperfiltration) and the effect of adipocytokines (leptin and aldosterone) to cause renal injury and fibrosis23,26. Leptin is an important determinant of the decline in eGFR in the general population, and mineralocorticoid receptor antagonists ameliorate the progression of CKD23,27. In the SUMMIT trial, decreases in estimated BV at 52 weeks (potentially related to the suppression of adipocytokines) were associated with reduction in albuminuria, but we observed no relationship with the improvements in eGFR. Tirzepatide tended to worsen eGFR estimated using cystatin C compared with placebo at 12 weeks, but this was reversed by 52 weeks, an effect that was consistently observed across all formulas used to determine eGFR. This pattern of an early worsening of eGFR followed by favorable improvements with longer-term follow-up was also observed in the tirzepatide versus insulin glargine in type 2 diabetes and increased cardiovascular risk (SURPASS-4) trial with tirzepatide28 and the Evaluate Renal Function with Semaglutide Once Weekly (FLOW) trial with semaglutide29, as well as other renoprotective drugs such as sodium–glucose cotransporter 2 inhibitors30. The present study suggests that the bimodal relationship may be explained by a relatively early-onset reduction in systolic BP and estimated BV, resulting in short-term decline in eGFR at 12 weeks. This is then superseded by a favorable effect on eGFR and UACR, potentially mediated by long-term decrease in fat mass and the suppression of adipocytokines.
Improvements in kidney function with incretins have been postulated to be related to a decrease in systemic inflammation, but we observed no correlation between changes in CRP and changes in eGFR. Systemic hypertension has been linked to the development of obesity-related CKD26, but we observed a direct relationship between decreases in systolic BP and decreases in eGFR at multiple time points. This may reflect the impact of reductions in renal perfusion pressure that have been associated with reduction in eGFR in both acute and chronic HF30,31. Tirzepatide reduced albuminuria compared with placebo, with a significant effect at 24 weeks, preceding the improvement in eGFR, which is also consistent with a decrease in glomerular hypertension as a key mechanism.
Tirzepatide reduced cardiac injury, reflected by decreases in troponin T, and reduced wall stress, reflected by decreases in NT-proBNP. The latter is notable because weight loss in the absence of HF leads to increases in NT-proBNP32,33. We did not require elevated NT-proBNP as an eligibility criterion, and thus, NT-proBNP levels in SUMMIT were only slightly elevated on average (median 175 ng l−1), and accordingly, there was little margin for further reduction. Circulating troponin levels are commonly elevated in HFpEF, where they are associated with greater risk for HF hospitalization or death14. The low-grade myocardial injury in HFpEF as observed at baseline in SUMMIT is believed to be related to cardiomyocyte loss due to repetitive elevations in cardiac filling pressures during stress, along with adverse loading conditions caused by ventricular–vascular stiffening13,34. Patients with HFpEF and elevated troponin have more severe elevation in filling pressures, reduced myocardial stress reserve and poorer exercise capacity compared with those without injury13, and individuals with the obesity phenotype have higher troponin levels than those without obesity15. We observed a modest but significant correlation between decreases in CRP and reductions in troponin with tirzepatide, suggesting that anti-inflammatory effects may contribute to cardiac benefits. It is noteworthy that the temporal sequence of anti-inflammatory effects and the changes in troponin were similar, and these were delayed compared with effects on circulatory volume and pressure, further supporting a distinct mechanism. The favorable effects of tirzepatide on myocardial injury may contribute to reduced risk for worsening HF seen in the SUMMIT trial16. Reduction in CRP with tirzepatide was also associated with greater improvement in 6MWD. This may relate in part to myocardial benefits, as noted above, or potentially improvements in skeletal muscle function and peripheral oxygen uptake, which are more dramatically impaired in patients with HFpEF and more severe inflammation35.
The major limitation of this analysis centers on the fact that we estimated PV using a weight-based formula (the Kaplan–Hakim equation)36, and according to this formula, the weight loss produced by tirzepatide would be mathematically expected to reduce PV. However, such an effect is physiologically inescapable, since PV/BV is inherently linked to body weight37, and thus, PV/BV necessarily declines as weight is lost. The mechanism that mediates this effect is probably due to a decrease in fat mass to reduce the secretion of adipocytokines that have antinatriuretic effects. However, in the case of tirzepatide, it is noteworthy that glucagon-like peptide-1 receptor agonism produces a direct effect itself to promote urinary sodium excretion, independent of changes in adipose tissue volume38,39. We understand that weight-independent formulas to estimate changes in PV have been proposed40, but these are relevant only for short-term interventions and are not applicable when there are meaningful changes in weight over months. Nevertheless, it is possible that we may have overestimated the magnitude of BV and PV reduction with tirzepatide in our analysis, as the relationship between BV and body weight may change as people lose weight. An alternative and more quantitative approach would be to directly measure PV/BV using the indicator-dilution method, but that would not be practical in a large-scale, international, multicenter randomized trial, leaving us no viable alternatives to explore this potential mechanism. All outcomes and analyses were prespecified, with the exception of the estimated BV and PV, as well as the regression analyses used to explore potential mechanisms, so these data should be treated as hypothesis-generating. Patients with active chronic noninflammatory myopathy and myositis may have mild elevation in troponin T independent of myocardial injury41. However, patients with significant musculoskeletal disease were excluded from SUMMIT by protocol. Reductions in body weight with tirzepatide would be expected to reduce skeletal muscle to some extent, which could influence creatinine dependent of changes in kidney function, and for this reason, we calculated eGFR using cystatin C in place of creatinine. Importantly, the findings showing kidney benefits were consistently observed across all formulas used to calculate eGFR. The duration of follow-up assessments for most measures was 52 weeks, reducing our ability to reach conclusions about longer-term effects.
In this mechanistic analysis from the SUMMIT trial, we show that tirzepatide reduced circulatory volume–pressure overload and systemic inflammation in patients with obesity-related HFpEF, while mitigating cardiovascular–kidney end-organ injury and loss of function. These data provide new insights into the mechanisms of benefit from tirzepatide in patients with obesity-related HFpEF.



Comments (0)