
Remember me





We retrospectively identified 79 patients with IDH-mutant astrocytoma with CDKN2A/B homozygous deletion treated among five distinct institutions (Massachusetts General Hospital, USA (n = 13); Dana Farber Cancer Institute, USA (n = 16); University Hospital Heidelberg, Germany (n = 34); University Hospital Dresden, Germany (n = 6); and Fudan-Shanghai, China (n = 10)) diagnosed between 1993 and 2023 (Table 1). Importantly, only cases in which CDKN2A/B deletion was identified at initial diagnosis were included. Patient demographics were similar among the cohorts, which was 58% male and had a median age at diagnosis of 36.2 years (Table 2), consistent with what has been previously reported [14, 15]. Of note, there were differences in patterns of administration of adjuvant therapy among institutions (Table 1).
Table 1 Characteristics of patients with IDH-mutant astrocytoma with CDKN2A/B homozygous deletion across five institutions (N = 79). Abbreviations IQR, interquartile range; RT, radiation therapy; TMZ, temozolomide; n/a, not applicableAs described in Methods, we concurrently identified 51 patients from Massachusetts General Hospital with astrocytoma, IDH-mutant, WHO grade 4, in which the grade 4 designation was made by histologic features alone to serve as a comparison cohort. The median age of this comparison group was 37.9 years (35.0 years for CDKN2A/B intact, 39.4 years for CDKN2A/B unknown) and it was 63% male. Overall, the demographics of CDKN2A/B deleted, CDKN2/B intact and CDKN2/B unknown cohorts are well matched (Table 2).
Table 2 Cohort characteristics of patients with astrocytoma, IDH-mutant, WHO Grade 4, based on CDKN2A/B status. Abbreviations IQR, interquartile range; RT, radiation therapy; TMZ, temozolomide; NE, not evaluated; n/a, not applicablePatients in the comparison cohort with tumors that received a WHO Grade 4 designation based on histologic features only were more likely to have received adjuvant radiation, chemotherapy or combination of the two when compared to patients with CDKN2A/B - deleted tumors (Table 2). Notably, significantly more patients in the comparison cohort received adjuvant radiation and temozolomide combined compared to those in the CDKN2A/B - deleted cohort (100% vs. 81%, p = 0.001).
There was no significant difference in the incidence of preoperative contrast enhancement between the CDKN2A/B - intact cohort and the CDKN2A/B - unknown cohort (86.7% vs. 80.6%, p = 0.61). Interestingly, the incidence of preoperative contrast enhancement was significantly lower in the CDKN2A/B - deleted group compared to the comparison cohort (Tables 2 and 58.2% vs. 82.4%, p = 0.004).
Impact of CDKN2A/B homozygous deletion on overall and Progression Free SurvivalIn the cohort of 79 patients with IDH-mutant astrocytoma with homozygous deletion of CDKN2A/B followed for a median of 5.1 years with 45 events observed, the median OS was 5.0 years. The median PFS in this cohort, based on 54 progression events, was 3.0 years. In contrast, the median OS of the comparison cohort of 51 patients with tumors that received a WHO Grade 4 designation based only on histologic features was 10.1 years, with the median OS in the 15 patients with IDH-mutant astrocytoma without detectable CDKN2A/B deletion undefined, followed for a median of 3.9 years, while the median OS of the 36 patients with unknown CDKN2A/B status was 10.1 years, followed for a median of 10.8 years. Similarly, the median PFS in the comparison cohort was 5.0 years (3.3 years for CDKN2A/B - intact and 5.9 years for CDKN2A/B - unknown). Although a small number of cases in the CDKN2A/B - unknown group may have CDKN2A/B deletion, the outcomes of this comparison cohort are similar to what has been reported for CDKN2A/ B non-deleted cases by Shirahata et al. [4] and Appay et al. [6]. Compared to the tumors designated as grade 4 based on histologic features, CDKN2A/B homozygous deletion was associated with significantly shorter OS (HR 2.45, 95% CI 1.51–3.99, p = 0.0004) and PFS (HR 1.95, 95% CI 1.27–3.00, p = 0.0026) by log-rank analysis (Fig. 1A and B). Importantly, the significantly shortened OS and PFS observed in our large, international cohort are in agreement with what has been described previously for smaller, single country cohorts [4, 6], emphasizing generalizability to real-world scenarios.
Fig. 1
Kaplan-Meier curves of the effect of CDKN2A/B homozygous deletion on (A) overall survival and (B) progression-free survival. P-values represent significance level as determined by log-rank test
In a Cox Regression Multivariate Model adjusting for CDKN2A/B status, age, adjuvant treatment, extent of resection, and preoperative contrast enhancement, CDKN2A/B homozygous deletion remained strongly predictive of shorter OS (HR = 3.51, 95% CI 1.92–6.38, p < 0.0001; Table 3). Similarly, CDKN2A/B homozygous deletion was also associated with shorter PFS when adjusting for the same variables (HR = 2.35, 95% CI 1.41–3.90, p = 0.00095; Table 3). Because our cohort was heterogeneously treated, we went on to investigate OS and PFS specifically in patients who received adjuvant radiation therapy and chemotherapy to control for a possible influence from treatment. We identified 64 (81%) patients in the CDKN2A/B deleted cohort and 51 (100%) patients in the comparison cohort who received upfront treatment with radiation followed by adjuvant chemotherapy (Table 1). Within this group, CDKN2A/B homozygous deletion remained significantly associated with shorter OS and PFS on both univariate (OS: 4.6 vs. 10.1 years, p = 0.0003; PFS: 2.6 vs. 5.0 years, p = 0.0024; Fig. 2) and multivariate analysis (OS: HR = 3.21, 95% CI 1.75–5.86, p < 0.0001; PFS: HR = 2.25, 95% CI 1.35–3.74, p = 0.0019) (Table 4).
Table 3 Results from the Cox regression analysis of the overall and progression free survival of multicentered cohort (N = 130). * indicates p < 0.05Fig. 2
Kaplan-Meier curves of the effect of CDKN2A/B homozygous deletion in patients who received adjuvant radiation and chemotherapy on (A) overall survival and (B) progression-free survival. P-values represent significance level as determined by log-rank test
Table 4 Results from the Cox regression analysis of overall and progression free survival of patients treated with adjuvant radiation and chemotherapy (N = 115). * indicates p < 0.05Altogether, these survival data demonstrate the strong negative prognostic effect of CDKN2A/B homozygous deletion in IDH-mutant astrocytoma, even when controlling for key variables that are associated with survival.
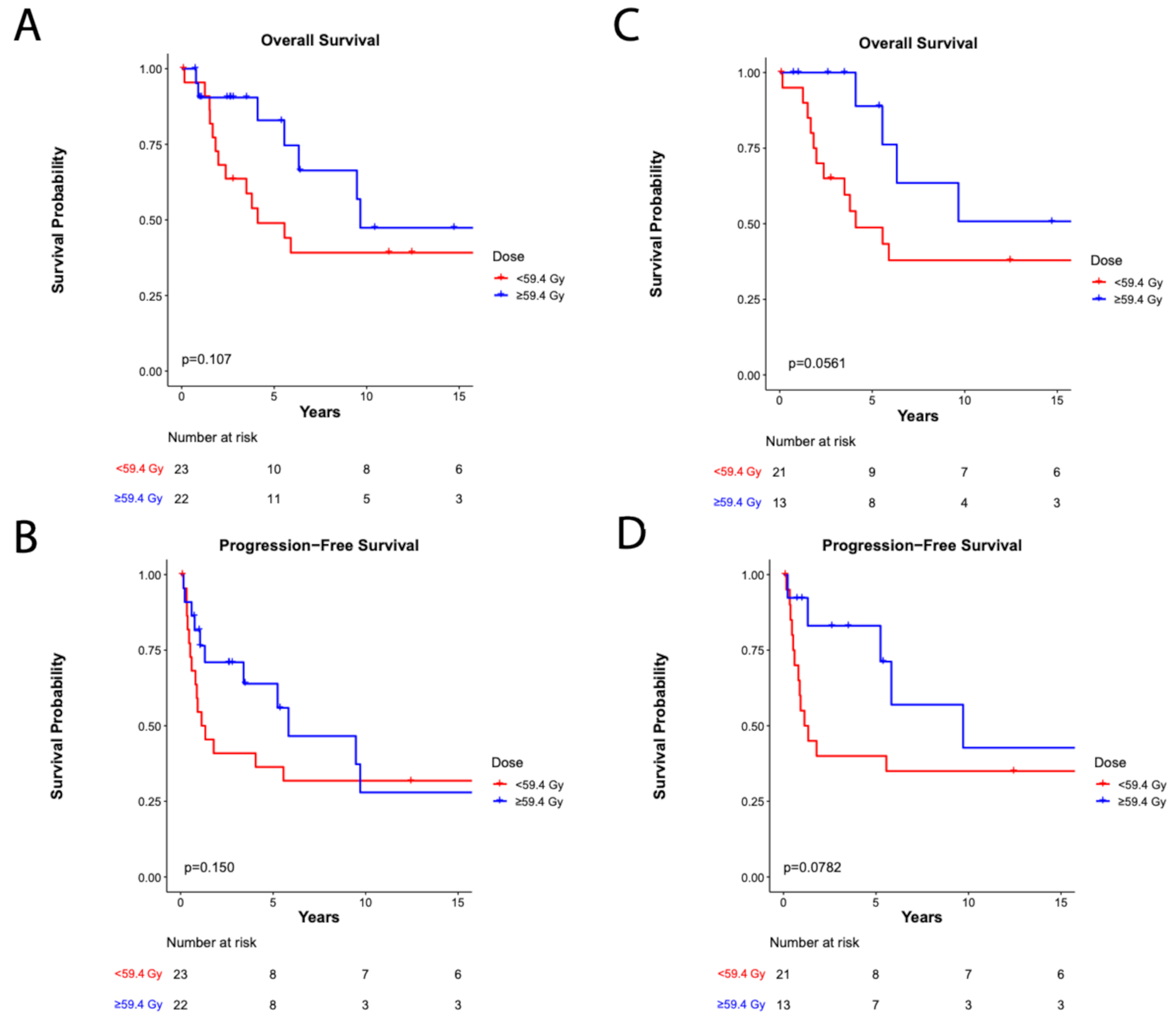
Predictors of survival within CDKN2A/B deleted patientsAlthough the impact of CDKN2A/B homozygous deletion on survival has been well demonstrated in the existing literature, radiographic predictors of survival within this subset of patients have not been thoroughly explored. Due to the previously reported association between preoperative contrast enhancement (CE) and poor survival outcomes in IDH-mutant glioma [16,17,18], we investigated whether CE was prognostic in our CDKN2A/B deleted cohort. CE, present in 46 (58%) of cases with CDKN2A/B homozygous deletion, was associated with shorter OS (4.0vs 7.3 years, HR 2.19, 95% CI 1.22–3.93, p = 0.0090) and PFS (2.2 vs. 3.3 years, HR = 1.74, 95% CI = 1.02–2.97, p = 0.0420) (Fig. 3). CE remained significantly associated with worse OS, but not PFS after adjusting for frontline treatment and age in Cox regression analysis (OS: HR = 2.49, 95% CI 1.17–5.28, p = 0.0176; PFS: HR = 1. 81, 95% CI = 0.98–3.36, p = 0.0588) (Table 5). In contrast, in the comparison cohort of tumors designated as WHO grade 4 by histologic features only, there was no association between preoperative contrast-enhancement and OS (HR 1.95, 95% 0.64–5.94, p = 0.239) or PFS (HR 1.40, 95% CI 0.59–3.34, p = 0.487). Overall, these data indicate that preoperative contrast-enhancement on MRI performed at initial diagnosis may be a significant predictor of shorter OS specifically with patients with CDKN2A/B deleted, IDH-mutant astrocytoma.
Fig. 3
Kaplan-Meier curves of the effect of pre-operative contrast enhancement on survival outcomes of patients with tumors with CDKN2A/B deletion (A / B) and comparision cohort with grade 4 determination made on histologic grounds (C / D). P-values represent significance level as determined by log-rank test
Table 5 Results from cox regression analysis of overall and progression free survival within patients with CDKN2A/B deletion (N = 79). * indicates p < 0.05
Comments (0)