
Remember me







Leg-Calve-Perthes disease is a genuine orthopedic enigma. While there is a consensus among pediatric orthopedic surgeons about the diagnosis of LCPD, there is no agreement regarding the treatment of patients. There is a general agreement that the prognosis is related to the age of the patient at disease onset. Patients who develop LCPD before the age of 5 years usually have a better prognosis and mostly do not need any intervention. On the other hand, the prognosis of patients who developed LCPD after the age of 8 years is substantially worse.1
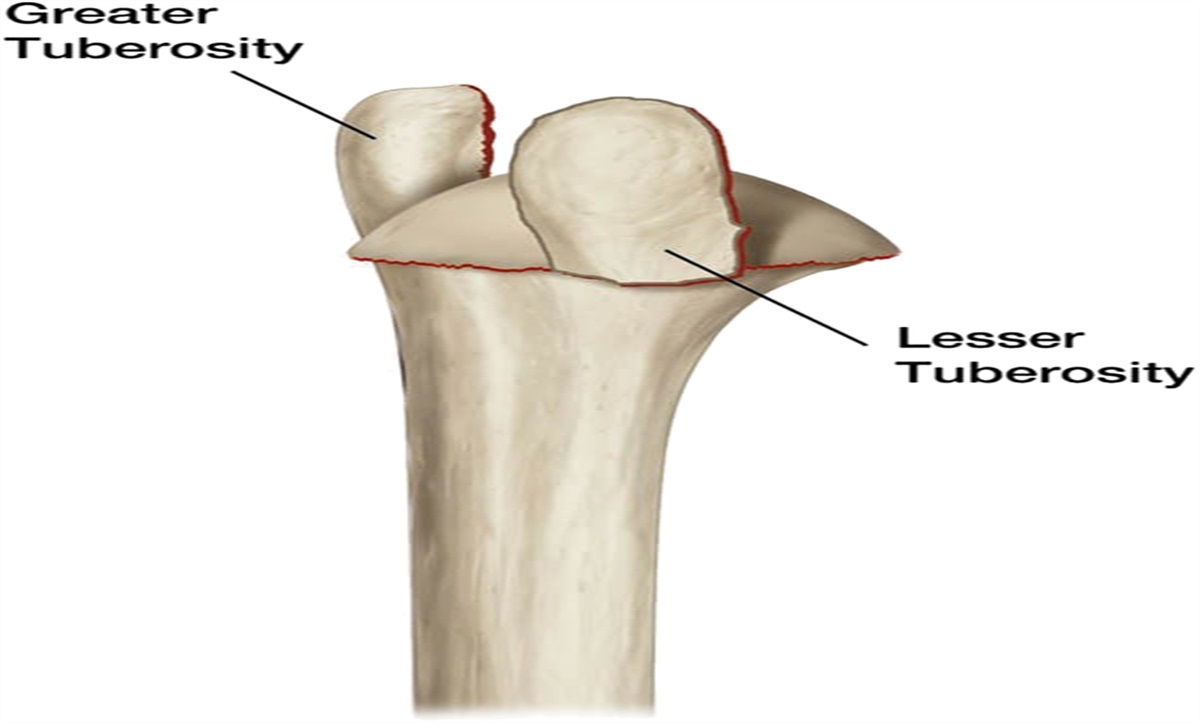
Stulberg classification is used to estimate the fate of the affected hip. There are 5 Stulberg types, where Stulberg 1 describes a round hip and acetabulum while Stulberg type 5 describes a relatively round acetabulum with a flat femoral head. The higher the Stulberg stage, the more compromised functional result is expected. Patients with higher Stulberg types have a higher chance of developing advanced hip arthritis and require hip replacement compared with lower stages. Usually, the natural history of patients who developed LCPD after the age of 8 years is an advanced Stulberg type. Those patients almost uniformly have coxa breva and overgrowth of the greater trochanter.2 Avascular necrosis of the femoral head causes flattening of the head and shortening of the femoral neck, while the GT is not affected by the disease process and continues its growth undisturbed. This eventually leads to a typical appearance of the hip at skeletal maturity (Fig. 1).
 FIGURE 1:
FIGURE 1: Coxa breva and magna and overgrowth of the GT of the right hip.
Over the last 10 years, we developed a minimally invasive treatment option for LCPD that we call a Rambam treatment protocol that includes:
Percutaneous adductor longus tenotomy Epiphyseal drilling of the area of the necrosis Closure of the GT Four months of non–weight-bearing of the affected legThe purpose of this study was to describe our experience with this protocol over the last decade.
MATERIALS AND METHODSThe study was approved by the Institutional Review Board.
Between the years 2011 and 2022, we treated 31 patients with LCPD. The average age was 7.1 years (range 5 to 10 years). All patients who presented to our institution and were diagnosed with LCPD were included. We divided the patients into 2 groups based on the Waldenström disease stage at presentation: group A included 18 patients at early fragmentation stage, group B included 12 patients in late fragmentation and one in reossification stage. All patients underwent the same treatment protocol as described.
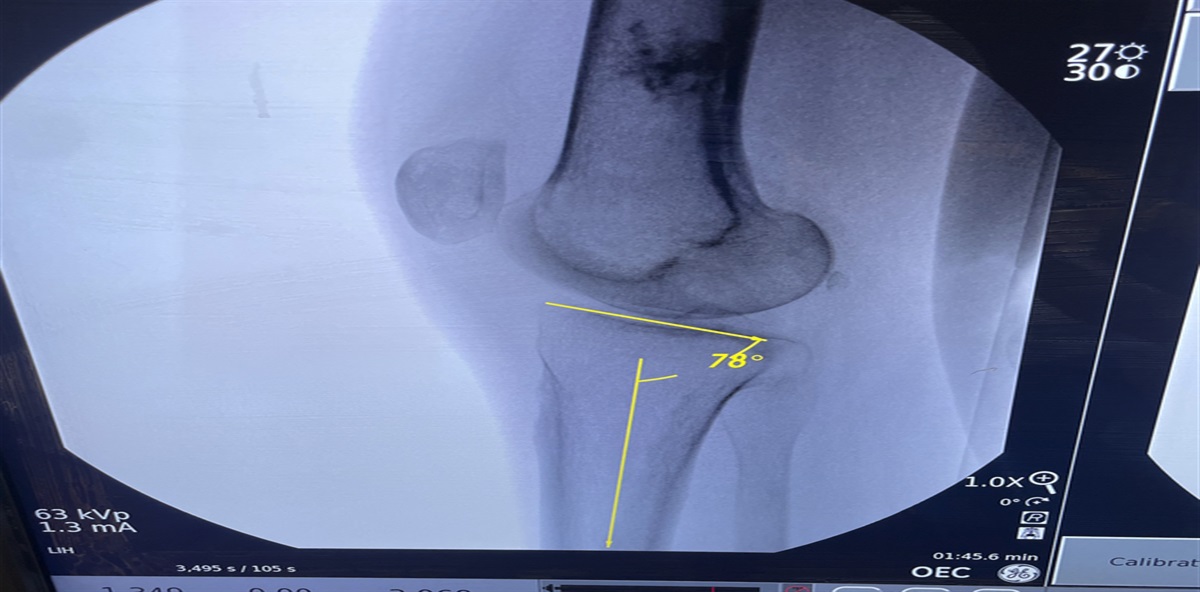
Operative TechniqueHip joint arthrography is always performed initially, which can be achieved through an adductor or a trochanteric approach. Based on our experience we usually prefer the latter as we feel that the trochanteric approach minimizes the spread of the contrast media into the soft tissues (Fig. 2A).
 FIGURE 2:
FIGURE 2: A: Arthrography of the hip joint, note the area of necrosis. B, Incision of only a few mm above the adductor longus at the level of inguinal crease. C, Ilizarov wire placed through the neck and into the center of the necrotic area. D, The wire is flipped with a blunt side leading toward the joint, thereby reducing the risk of wire advancement into the joint during drilling. E and F, Drilling using a cannulated drill over the wire. The drill should reach the necrotic area without penetrating into the joint.
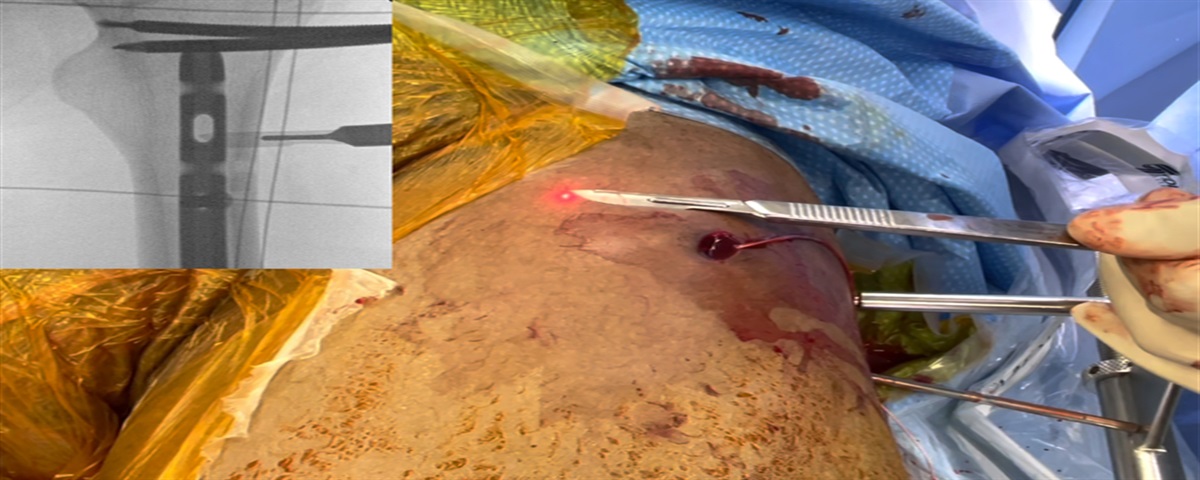
Step 1. Percutaneous Adductor Longus TenotomyIn many LCPD patients who have active disease, the adductor longus is commonly tight and may limit abduction. Our preferred technique for this step is a percutaneous tenotomy through a minimal incision (Fig. 2B).
Step 2. Transepiphyseal Drilling of the Necrotic Area in the Femoral EpiphysisThis is the main and most important part of the treatment protocol and should be done thoroughly. The necrotic area of the physis usually includes the anterolateral aspect of the epiphysis of the femoral head. The purpose of the drilling procedure is to decompress and increase vascularization of the necrotic area of the epiphysis. Thus, the drilling of the epiphysis should be done precisely in the center of the necrotic area. The necrotic area can usually be visualized after arthrography (Fig. 2A).
A 10-mm incision just below the GT is made. Via this incision, a 1.8-mm Ilizarov wire is introduced through the femoral neck and into the anterolateral aspect of the femoral head epiphysis. Position is assessed using fluoroscopy in 2 planes (antero-posterior view and frog view when the hip is flexed and abducted). The wire should be inserted up to the femoral head cartilage (but not cross the cartilage). Then, a cannulated 4.8 mm drill is used to drill over the wire up to the subchondral bone (Fig. 2C). Care should be taken not to enter the hip joint either with the wire or the drill (Figs. 2E, F). As the end of the Ilizarov wire is very sharp and tends to advance into the joint during drilling, we recommend exchanging the wire after drilling, placing the blunt end into the cavity to prevent migration (Fig. 2D). Thus, the chance of wire advancement into the joint is minimal if even possible. A wire crossing the joint can cause wire breakage, cartilage injury, and potentially even chondrolysis, and should be avoided.
Step 3. Closure of the Greater Trochanter ApophysisThrough the same incision used earlier for femoral head drilling, closure of the apophysis of the GT can be performed (Fig. 3A). Our preferred technique for GT apophysis closure involves introduction of a wire through the GT under fluoroscopy, followed by drilling over the wire, thereby destroying it. The same lateral cortical hole is used with a noncannulated drill to drill slightly anterior and posterior, thereby destroying the whole apophysis (Fig. 3B).
 FIGURE 3:
FIGURE 3: Closure of the GT through the same incision as the femoral drilling. A, The length of the incision for epiphyseal drilling and GT apophysis closure. B, Closure of the GT using a solid drill. Insertion of guidewire and drilling with a cannulated drill over the wire is also a viable option.
Postoperative ProtocolNon–weight-bearing of the affected leg is maintained for 4 months postoperatively. Children are encouraged to weight-bear with crutches on the contralateral side. Physiotherapy that includes full flexion, abduction, and internal and external rotation of the hip is crucial for the success of the treatment.
RESULTSA total of 31 patients were included in this study (Tables 1 and 2). Mean follow-up was 52 months. All patients had a limp before surgery. On the latest follow-up, 22 had no limp, 23 had substantial improvement in hip range of motions. In group A, 12 patients had Stulberg type 1, 5 Stulberg type 2, and 1 Stulberg type 3. In group B, 1 patient had Stulberg type 2, 9 patients had Stulberg type 4, and 3 patients had Stulberg type 5.
TABLE 1 - Patient’s Demographics and Radiographic Data—Group A N Age G Waldenström ST LP Stulberg 1 7 F EF A B 1 2 8 F EF A B 2 3 7 M EF B B 1 4 6 F EF — B 2 5 7 F EF — C 2 6 6 F EF — B/C 1 7 7 F EF B B 2 8 6 F EF B B 2 9 10 M EF B B/C 3 10 7 M EF — B 1 11 5 M EF A B 1 12 8 F EF B B/C 1 13 7 M EF B B 1 14 5 F EF A B/C 1 15 6 M EF — B 1 16 8 F EF — A 1 17 7 F EF B B/C 1 18 9 M EF B A 1Age, in years.
EF indicates early fragmentation; G, gender (M-male, F-female); LF, late fragmentation; LP, Herring lateral pillar classification; N, patient number; R, reossification; S, side (R-right, L-left), Waldenström stage; ST, Salter and Thompson classification.
Age, in years.
EF indicates early fragmentation; G, gender (M-male, F-female); LF, late fragmentation; LP, Herring lateral pillar classification; N, patient number; R, reossification; S, side (R-right, L-left), Waldenström stage; ST, Salter and Thompson classification.
The idea of transepiphyseal drilling in patients with LCPD is not new: Nuno Craviero Lopes3,4 performed it for many years in Portugal. In his experimental studies, he concluded that transepiphyseal neck-head drilling led to a marked increase in epiphyseal vascularization.
Closure of the GT is important to prevent overgrowth of the trochanter, eventually causing hip abductor weakness, limping, and a Trendelenburg gait. In our experience, closure of the GT by drilling, as described here, is the most effective and simple way to achieve GT apophysis closure. We found other techniques, like screws/staples fixation, to be less effective. While many agree that GT closure below the age of 8 years has an effect on GT growth, the need for GT epiphysiodesis for patients older than 8 years is controversial.5 Due to the minimal morbidity associated with our GT epiphysiodesis technique and considering the potential of GT growth even in patients older than 8 years,6 we recommend GT closure in all patients up to 10 years of age.
We believe that 4 months of non–weight-bearing is also an important part of the protocol. In our experience, this provides sufficient time for the epiphysis to heal after drilling. Shorter non–weight-bearing periods might lead to collapse of the subchondral bone, leading to cartilage damage. Longer periods, on the other hand, may cause osteopenia of the affected limb. We are fully aware that the joint reaction forces can also affected by muscle action around the hip joint; thus, they can be reduced by allowing touch weight-bearing instead of non–weight-bearing. Though, in our patient population we believe that simplicity is key. Compliance with postoperative instructions is challenging in this age group and minimal and simple instructions lead to better adherence. Thus, we limit our recommendations to non–weight–bearing and full active and passive range of motion.
Our results show that the protocol can be effective when implemented at early disease stages. On the other hand, when performed at later stages, it has minimal effect on remodeling, and the result is less satisfying. One of the main advantages of the proposed treatment is its minimally invasive nature and minimal morbidity associated with it. This treatment option does not interfere with any other treatment options if required in the future.
Illustrative CaseAn 8-year-old girl with severe restriction in hip motions of the left hip (Figs. 4A, B). The Rambam Protocol was performed close to presentation. At the last follow-up 3 years postoperatively, the hip presented was classified as Stulberg type 1 and identical epiphysial-trochanteric distance of both hips. Note that there is no Coxa Magna, no Coxa Breva and normal relation between the center of the femoral head and the GT on both sides.
 FIGURE 4:
FIGURE 4: A and B, 8-year-old girl with left LCPD. C and D, 3 years after epiphyseal drilling and closure of the GT. Note that epiphyseal-trochanteric distance is preserved, no coxa magna and breva, no overgrowth of the GT, and hip is Stulberg type 1.
CONCLUSIONSOn the basis of our experience, the Rambam Protocol may be an effective treatment in patients in the early stages of LCPD. This protocol has become our routine for the treatment of early stages of LCPD.
REFERENCES 1. Ippolito E, Tudisco C, Farsetti P. The long-term prognosis of unilateral Perthes’ disease. J Bone Joint Surg Br. 1987;69:243–250. 2. Stulberg SD, Cooperman DR, Wallensten R. The natural history of Legg-Calve-Pethes disease. J Bone Joint Surg Am. 1981;63:1095–1108. 3. Lopes NC, Escalada C. Prevention of Legg-Calve-Perthes disease, transepiphyseal neck-head drilling. Rev Port Orthop Trauma. 2011;19:223–238. 4. Eidelman M, Kotlarsky P. Does transepiphyseal drilling and closure of the greater trochanter in early Legg-Calve-Perthes disease improve natural history? Musculoskeletal Surg. 2023;107:279–285. 5. Kwon KS, Wang SI, Lee JH, et al. Effect of greater trochanteric epiphysiodesis after femoral varus osteotomy for lateral pillar classification B and B/C border Legg-Calvé-Perthes disease: A retrospective observational study. Medicine (Baltimore). 2017;96:e7723. 6. McCarthy JJ, Weiner DS. Greater trochanteric epiphysiodesis. Int Orthop. 2008;32:531–534.
Comments (0)