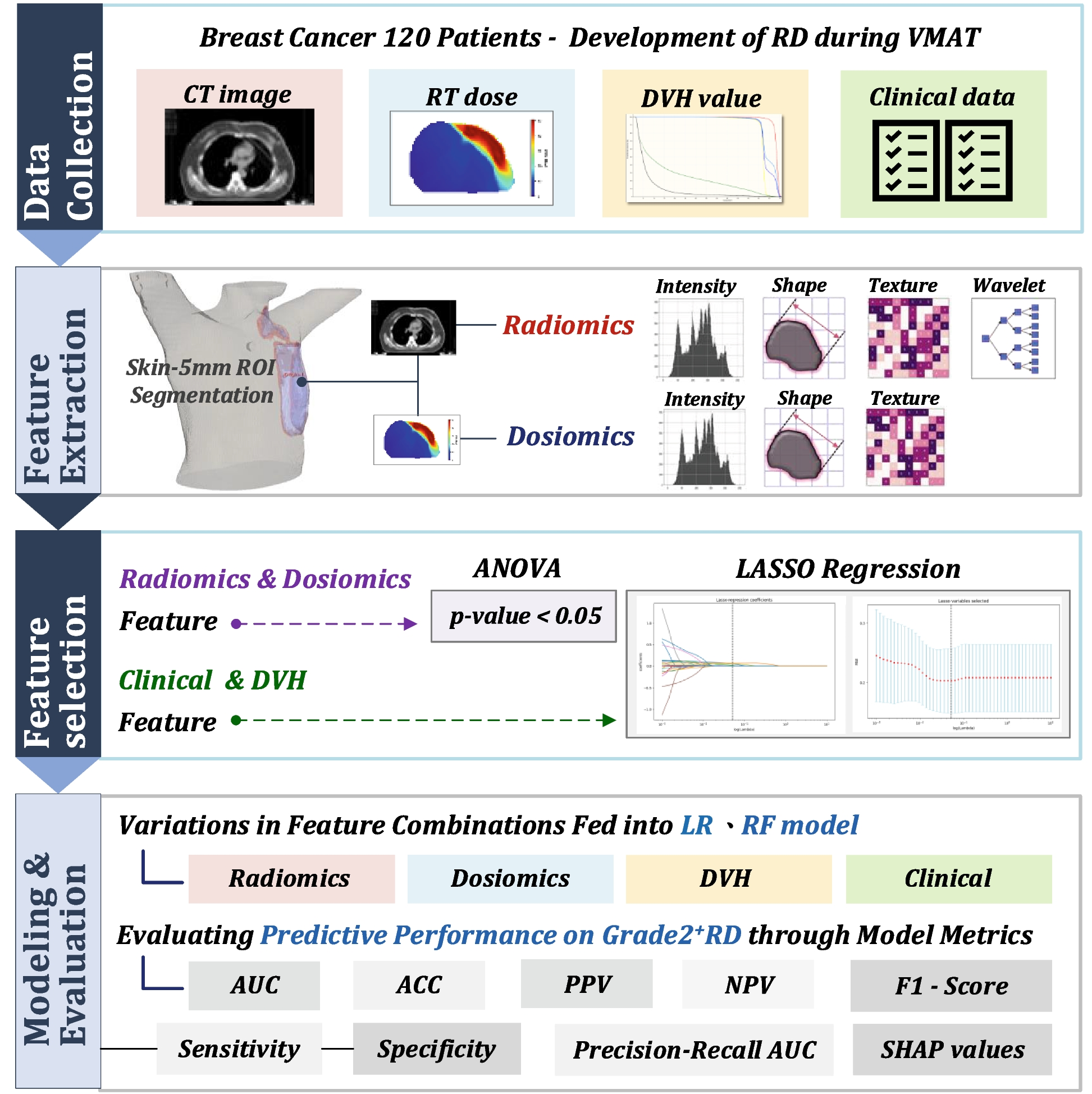
Currently, there are relatively few studies utilizing Radiomics and Dosiomics methods for predicting RD responses in breast cancer patients based on CT images. Therefore, this research aims to delve deeper into the potential of Radiomics and Dosiomics approaches for predicting more severe RD responses in breast cancer patients through the analysis of predictive model results from 10 different feature subsets. This exploration seeks to understand whether these methods can offer broader assessments and contributions towards forecasting the severity of RD reactions in such patients.
From the AUC metrics presented in Fig. 3(b), the RF model's performance metrics underscore its robustness in predicting Grade 2+ RD. The best-performing feature subset I, which includes Clinical, Radiomics, and Dosiomics features, achieved an AUC of 0.83, closely followed by subset F, consisting solely of Radiomics and Dosiomics features, with an AUC of 0.81. These results highlight the significant contribution of Radiomics and Dosiomics features in enhancing the prediction of Grade 2+ RD in breast cancer patients. Comparatively, the RF model generally exhibited higher average accuracy and PPV than the LR model across all feature subsets, indicating a potential overall performance advantage in predicting Grade 2+ RD. Notably, in the Precision-Recall AUC metric, the LR model's Subset I and the RF model's Subset J performed exceptionally well, achieving an optimal balance between precision and recall.
Given the RF model's superior performance across most metrics, it is recommended for predicting Grade 2+ RD in breast cancer patients. This recommendation is further supported by the findings of Feng et al. [18], who reported that models using clinical and dosimetry parameters alone, Radiomics features alone, and a combination of all three resulted in validation set AUCs of 0.816, 0.907, and 0.911, respectively. These figures corroborate the substantial role of Radiomics features in boosting the predictive accuracy for Grade 2+ RD, demonstrating the effectiveness of integrating these advanced imaging and dosimetry analyses for more accurate and reliable RD risk assessments.
Although the AUC of feature subset G (comprising Clinical, DVH parameter, and Radiomics features) achieved 0.78 in LR and 0.72 in RF models in this study, which is lower compared to the AUC of 0.911 for a similar feature combination reported by Feng et al. [18], this discrepancy can be attributed to several factors. Differences in sample sizes, definitions of RD timing, feature selection and ROI planning, data preprocessing, algorithms, hyperparameter settings, patient characteristics, and sample proportions are among the various details that may lead to these variances [17]. Such differences underscore the complexity of modeling and the impact of methodological variations on the performance of predictive models.
RD is a non-stochastic effect where the severity can increase proportionally with the magnitude of the dose received. This notion is supported by studies from Xie et al. [23] and Vicini et al. [24], which highlighted that breast volume significantly influences the incidence of RD following RT in breast cancer patients. Correspondingly, in this study, the LASSO results for the optimal feature subset I, as depicted in Fig. 4, predominantly selected features from the Radiomics and Dosiomics categories that focus on skin areas receiving 100% and 105% of the prescribed dose (PTV100% and PTV105%). This alignment of findings emphasizes the critical role of dose intensity and affected volume in the development of RD.
The LASSO method was utilized to filter out Radiomics and Dosiomics features significantly correlated with the prediction of Grade 2+ radiation dermatitis (RD) in breast cancer patients. The selected multidimensional features include texture, shape, and first-order statistical features. According to the results depicted in Fig. 4, Radiomics features, predominantly those transformed by wavelet filters (20 features), were selected due to their potential association with cellular damage, vascular changes, or other structural alterations within the region [25]. Wavelet-filter transformations in our study enhance feature extraction by capturing information at multiple resolutions, which is crucial for identifying texture features. These features, indicative of subtle underlying tissue changes, are revealed through variations in high-frequency and low-frequency signals across different scales and orientations. High-frequency details may correspond to fine structural changes like cellular damage or minor vascular alterations, while low-frequency content often reflects broader anatomical features such as blood vessels [26].
The utility of wavelet-transformed features is particularly noted in their ability to detect changes at the lesion margins from high-frequency signals in the images. This capacity for capturing fine details associated with structural changes in tissues suggests potential pathological alterations, making wavelet transformations valuable in medical image analysis for distinguishing various physiological and pathological conditions [26]. However, it's crucial to recognize that the assumption that these features directly represent specific tissue changes remains theoretical. We have not yet empirically validated a direct correlation between wavelet-transformed features and specific tissue alterations like cell damage or vascular changes. Consequently, interpretations should be made with caution. Future research should focus on linking these radiomic features with histopathological findings and clinical outcomes to confirm their predictive effectiveness for radiation dermatitis, ensuring the scientific integrity of our findings and guiding clinical applications.
The Radiomics features most highly correlated with Grade 2+ RD were identified as Radiomics_skin5mm_v45_wavelet-HLL_glcm_InverseVariance and Radiomics_ptv_105_wavelet-LHL_glcm_InverseVariance, where the glcm_InverseVariance feature evaluates the consistency of grayscale values within the image region. This observation suggests that uniform tissue texture in the skin regions of breast cancer patients may reduce their susceptibility to developing moderate to severe RD. While direct evidence linking consistent tissue texture to lower RD incidence is sparse, this concept aligns with findings from Feng H’s study [18]. The study indicates that repositioning PTV and skin regions to areas with a lower prevalence of radiomic features associated with moderate to severe RD could potentially lessen the occurrence of these conditions [18]. This supports the hypothesis that homogeneous radiomic characteristics across these regions might positively impact RD outcomes.
Regarding the selected Dosiomics features, since this study did not enhance images with filters before extracting Dosiomics features, the original dose-related features were selected. Dosiomics_ptv_100_original_glszm_SizeZoneNonUniformity reflects the non-uniformity of the radiation dose distribution in the PTV100% area based on dose texture, which may lead to localized tissue receiving higher than expected radiation doses, increasing the risk of Grade 2+ RD. The feature Dosiomics_ptv_100_original_glrlm_HighGrayLevelRunEmphasis might also indicate that areas of the skin exposed to higher doses are associated with an increased risk of Grade 2+ RD.
This result suggests that besides dose levels, the uniformity and texture consistency of skin tissue are crucial factors affecting the occurrence of RD, which can vary among patients. In this study, we derived Dosiomics features and DVH parameters from RT-DOSE files exported from the TPS, utilizing these data to assess the impact of radiation exposure relevant to our analysis of RD.
In this study, the performance of the various feature subsets, as shown in the model results of Fig. 2, indicates that the least effective feature subset A, which has been a common combination in many previous studies on predicting complications, achieved an AUC of only 0.62 in this study. Subset A is composed of clinical information of breast cancer patients and DVH dose parameters calculated by TPS. This may be precisely because the skin dose calculated by TPS is not accurate, preventing the model from learning to predict whether a patient will develop Grade 2+ RD based on the dose information received by the skin accurately. However, the model results of subsets incorporating Radiomics and Dosiomics features, such as subset D (AUC = 0.73), subset E (AUC = 0.71), subset G (AUC = 0.78), and subset H (AUC = 0.72), demonstrate that combining DVH parameter features with Radiomics and Dosiomics features can effectively enhance the prediction of Grade 2+ RD in breast cancer patients. Among these, subsets D and G, which incorporate Radiomics features, compared to subsets E and H that include Dosiomics features, further highlight Radiomics' superior assistance in prediction. Overall, these findings may have significant implications for improving radiation treatment planning and reducing the incidence of RD.
The multivariate analysis of the clinical characteristics of the 102 breast cancer patients included in this study and their relationship with RD, as shown in Table 1 and Fig. 4, indicates that laterality, type of surgery, AJCC cancer staging, SCF, IMN, and whether chemotherapy was received are not significantly related to the occurrence of Grade 2+ RD in this study.
Numerous studies have observed a correlation between higher BMI values and the incidence of more severe RD [6, 27,28,29], consistent with the results of the ANOVA statistical test (p-value < 0.05) in this study. However, no significant correlation was observed during the LASSO feature importance analysis. This discrepancy may be attributed to the average BMI values of both groups in this study's sample not exceeding 25 (Grade 2+ RD: 24.74, < Grade 2+ RD: 23.2), suggesting a lower prevalence of overweight and obese patients, who are typically beyond the standard BMI range.
Our study highlights the correlation between age and the incidence of Grade 2+ RD, supported by both ANOVA and LASSO regression analysis, aligning with findings from Córdoba et al. [30], which noted increased severe skin toxicity in older women. This suggests that aging may reduce physiological resilience, like blood flow and DNA repair, enhancing susceptibility to severe skin reactions. Conversely, broader research, including studies referenced [7, 27], generally shows minimal correlation between age and RD severity, pointing to potential influences from sample demographics, size, and feature distribution in the analysis, which might introduce inconsistencies in findings.
In analyzing the influence of various features on RD prediction, Figs. 5 and 6 provide crucial insights into the SHAP value comparison between the LR and RF models. The LR model highlights age as a significant factor affecting RD risk, with SHAP values ranging from -0.2 to 0.4, suggesting that older age groups are more likely to develop Grade 2+ RD. In contrast, the RF model shows a more uniform distribution of feature impacts across all features, with age impact values ranging from -0.05 to 0.05, indicating a more balanced and robust integration of predictors across diverse clinical scenarios. This balanced feature influence enhances the RF model's potential for stable predictions. Moreover, the feature 'R_skin5mm_v50_wavelet-HLL_glcm_InverseVariance' stands out in both models, underscoring the importance of textural uniformity in the skin area receiving 50 Gy, processed through wavelet transformation. This feature's significant impact in both models highlights its crucial role in predicting RD, emphasizing how texture uniformity correlates with radiation response.
Every breast cancer patient undergoing RT is fitted with a custom thermoplastic mold to ensure proper immobilization and repeatability. This setup may lead to an increase in the surface dose of the breast [31, 32]. In previous studies, this aspect was not considered [7]. In response, the current practice adjusts for this by deducting 3 mm for the thermoplastic mold when calculating and planning the ROI for Radiomics and Dosiomics within the TPS, establishing a baseline for the actual skin of the patient.
Furthermore, considering the epidermal, dermal, and subcutaneous layers of the skin [33], and based on findings by Hälg et al. [34] that the vascular distribution in the skin is approximately at an average depth of about 5 mm, this study aims to preserve the vascular tissues of the patient's skin to maintain its functionality. Thus, the ROIs for the skin areas of patients are delineated with a thickness of 5 mm below the actual skin.
In this study, we did not specifically address data imbalance, where 33 patients experienced RD and 69 did not, to maintain the authenticity of the dataset and reflect real clinical scenarios. Using VMAT provides effective dose control, thus naturally resulting in a lower incidence rate of RD. We utilized stratified k-fold cross-validation in our training processes to maintain consistent class ratios, partially mitigating the impact of imbalance. Moreover, we conducted repeated tenfold cross-validations to ensure model stability and reliability. The RF model, which performs well in handling data imbalances, showed promising results. These approaches helped reduce the potential negative effects of the imbalance on model performance while keeping the dataset representative of the clinical environment.
This study also has some limitations and constraints. Firstly, the relatively small sample size and the overall proportion of toxic endpoints might affect the results of statistical analysis, suggesting that future studies with larger sample sizes are needed to validate these findings. The application of Radiomics and Dosiomics methods in observing the development of RD toxicity in breast cancer patients is still limited. Moreover, the delineation of ROI conducted by different professionals such as physicians and physicists may introduce variability, which was not accounted for in this study.
Future research will focus on integrating our predictive model for RD into clinical workflows, significantly enhancing treatment planning and patient management in the field of radiation oncology. The plan involves embedding the model directly into existing TPS, enabling oncologists to assess RD risk in real-time and adjust treatment parameters based on individual patient risk profiles. This strategy not only allows for personalized treatment adjustments, such as dose fractionation and advanced skin-sparing techniques, especially for high-risk patients, but also supports real-time monitoring during treatment. This facilitates proactive treatment adaptations and improves communication with patients regarding potential side effects. Post-treatment, the model aids in identifying patients who require early dermatological intervention, thus enhancing care outcomes. As treatment outcome data continue to be collected and analyzed, this will further refine the model’s accuracy and reliability, making it a valuable tool for enhancing the precision and efficacy of radiation therapy in clinical settings. Additionally, future research will explore how to leverage this model to support broader clinical environments, promoting more personalized and effective patient management.


Comments (0)