
Remember me





Pediatric extracorporeal membrane oxygenation (ECMO) patients require anticoagulation to inhibit hemostatic activation and prevent thrombosis when circulating blood encounters the foreign surface of the ECMO circuit, but treatment may contribute to bleeding complications, which are reported in 70% of pediatric ECMO patients and associated with increased mortality (1–3). The most widely used systemic anticoagulant during ECMO is unfractionated heparin (UFH) (4,5). UFH has a long history of use in the pediatric ECMO population and its advantages include low cost, short half-life, full reversibility, wide access to laboratory monitoring tests, for example, activated partial thromboplastin time, and clinician familiarity with use (6). Disadvantages include variation in patient response to fixed dosing, heparin resistance related to variable plasma binding, and variable sensitivity to the effect of antithrombin (AT) in younger children (7,8). UFH does not inhibit thrombus-bound or platelet-bound thrombin while direct thrombin inhibitors (DTIs; bivalirudin, argatroban, lepirudin) inhibit both free and bound thrombin, and are AT-independent providing a greater inhibition of thrombin than does UFH (9). Bivalirudin has been used in pediatric patients with heparin-induced thrombocytopenia (HIT), heparin resistance, and continued thrombosis despite heparin therapy during ECMO (10), and as a first-line agent in some centers.
Evidence to guide optimal choice of anticoagulant medication(s) in pediatric ECMO is limited. The objective of this subgroup of the Pediatric ECMO Anticoagulation CollaborativE (PEACE) was to derive a systematic-review informed, modified Delphi consensus regarding the selection of anticoagulant medications during pediatric ECMO support.
MATERIALS AND METHODSDetailed methods and definitions of clinically relevant bleeding are described in the PEACE executive summary (11). Briefly, a structured literature search was performed using PubMed, EMBASE, and Cochrane Library CENTRAL databases from January 1988 to May 2020, with an update in May 2021. Literature on alternate medications for anticoagulation and their impact on patient outcomes were reviewed (Supplemental Methods, https://links.lww.com/PCC/C495). Two authors reviewed all citations independently, with a third independent reviewer resolving any conflicts. Evidence tables were constructed using a standardized data extraction form (11). Risk of bias (RoB) was assessed using the Quality in Prognosis Studies (QUIPS) tool or the revised Cochrane RoB for randomized controlled trials, as appropriate (12–14), and the evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system (15,16). A panel of 48 experts met over the course of 2 years to develop evidence-based recommendations and, when evidence was lacking, expert-based consensus statements, or good practice statements for anticoagulant medications. The supporting literature was reviewed and statements were developed using the Evidence to Decision framework, emphasizing the panel’s assessment of risks versus benefits of each proposed statement and a prioritized list of patient outcomes that had been created by a web-based survey of expert panel members (17–19). A web-based modified Delphi process was used to build consensus via the Research and Development/University of California Appropriateness Method (20,21). Consensus was defined as greater than 80% agreement. Additional references, not included in the structured literature search, were included in rationale statements to provide context but were not used to derive recommendations, or consensus statements, or good practice statements.
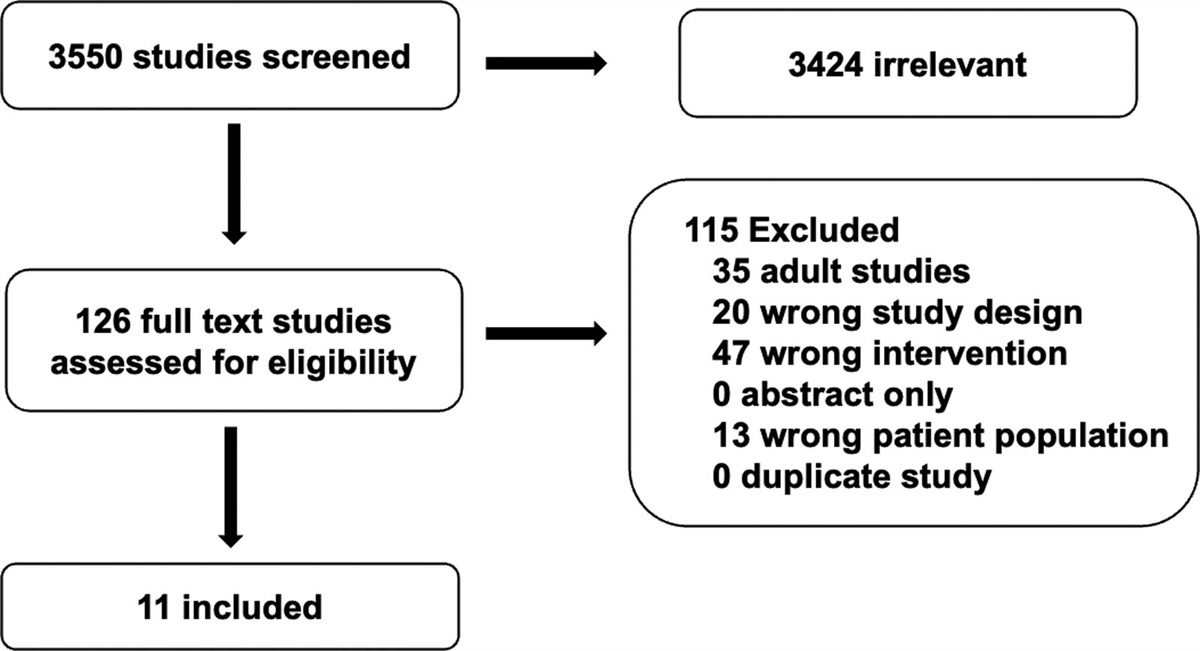
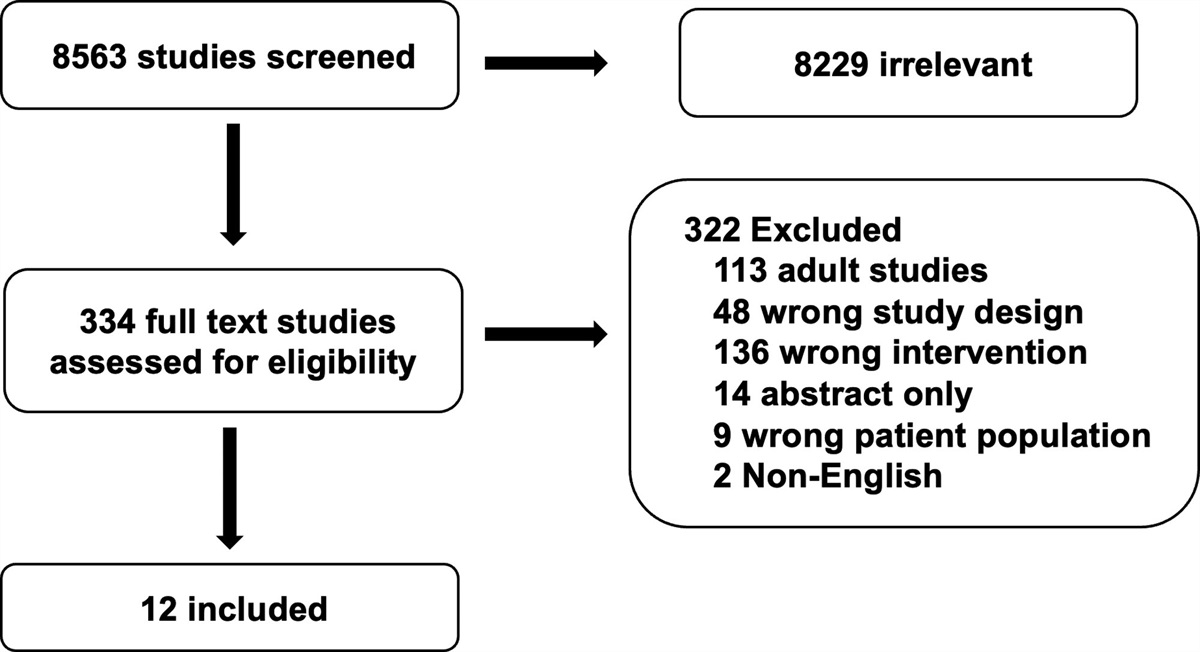
RESULTSThe structured literature search identified 8283 abstracts. Evaluation of these led to exclusions of 7786 references. An additional 479 references were excluded based on a full article review, leaving a final tally of 18 references that were used for recommendation and consensus statement creation (Fig. 1). The included references are detailed in Supplemental Table 1 (https://links.lww.com/PCC/C495). A summary of RoB assessments is in Supplemental Figure 1 (https://links.lww.com/PCC/C495). Two recommendations, two consensus statements, and one good practice statement were developed, and in all, an agreement greater than 80% was reached.
 Figure 1.:
Figure 1.: Depicts the Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram of studies screened and included in the anticoagulant medication during pediatric extracorporeal membrane oxygenation subgroup.
Provision of Systemic Anticoagulation Consensus Statement2.1 It is reasonable to consider that anticoagulation be administered during pediatric ECMO, which may be reduced or held in specific cases when clinically significant bleeding exists, but the risks of circuit clotting (especially in low flow conditions) must be weighed against potential benefit.Consensus panel expertise with weak agreement, 91% agreement (n = 44), median 8, interquartile range [IQR] 7–9.
Summary of the evidence:There are no pediatric studies suggesting ECMO should be provided without systemic anticoagulation, although small case series in patients with severe hemorrhage exist. More evidence for this practice exists in the adult ECMO population (22,23). These reports include patients with short ECMO duration without anticoagulation (24–26). Adult patients on ECMO have larger cannulas and higher ECMO flow than small children, and these factors may influence the risk of clotting during ECMO. Although there are pediatric case series reported, in whom anticoagulation is withheld, the numbers are small and patients are not compared with those receiving systemic anticoagulation. In one case series of four pediatric patients with severe hemorrhage, systemic anticoagulation was held for a median of 10 hours. One patient survived. In the three deaths, no significant thrombus was found on autopsy (27).
Balance of benefits versus harms:Although cessation of systemic anticoagulation in patients with severe hemorrhage or other risk factors may be feasible, further investigation to evaluate the benefits or limitations of this practice with strictly defined goals and study factors in a pediatric population is needed.
Unfractionated Heparin and Direct Thrombin Inhibitors Recommendation2.2 There is insufficient evidence to recommend bivalirudin as a first-line anticoagulant in pediatric ECMO.Weak Recommendation, very low-quality pediatric evidence, 89% agreement (n = 44), median 8, IQR 7–9.
Consensus Statement.2.3 It is reasonable to consider bivalirudin as an alternative to UFH for select clinical scenarios and/or in centers with experience in use and monitoring.Consensus panel expertise with weak agreement, 89% agreement (n = 44), median 8, IQR 7–9.
Summary of the evidence:The routine use of bivalirudin for children with ventricular assist devices (VADs) has been established (28,29); however, data supporting the routine use in children on ECMO is limited to single-center reports. In a prospective observational pediatric ECMO study, Ryerson et al (30) reported outcomes in 18 children anticoagulated with bivalirudin. In this mainly cardiac surgical population, 80% of the patients had been started on UFH and transitioned to bivalirudin due to presumed heparin resistance or ongoing circuit thrombosis despite therapeutic anti-factor Xa (anti-Xa). They found a lower rate of circuit intervention in patients receiving bivalirudin compared with those receiving UFH, and no increased thrombotic complication. However, four patients had significant bleeding, including intracranial bleeding (n = 2) and postprocedural bleeding (n = 2). Studies comparing blood loss (31,32) between the therapeutic agents yield mixed results. One study found significantly higher blood loss because of laboratory sampling in the UFH group compared with the bivalirudin group, but no difference in blood product exposure (32). Other similar small, single-center studies have shown no difference in outcomes of circuit interventions, transfusions, or survival to hospital discharge (33,34). Studies of resource utilization in children managed on ECMO with bivalirudin or UFH suggest that even when allowing for the lower daily cost of UFH, the use of bivalirudin resulted in cost savings when the associated cost of care (e.g., AT replacement and laboratory testing) were included (35,36).
Snyder et al (37) reported 98% survival without significant bleeding or thrombosis in 42 neonates with a congenital diaphragmatic hernia (CDH) supported with venoarterial ECMO and standardized anticoagulation with bivalirudin as the primary anticoagulant. These results suggest that bivalirudin can be used in neonates undergoing CDH repair with minimal complications. Conclusions, however, are limited due to the retrospective nature and lack of a comparison group.
These small, single-center, observational studies (total n = 159 pediatric patients exposed to bivalirudin on ECMO) suggest bivalirudin may be a reasonable alternative anticoagulant for patients with clinical indications including HIT, heparin resistance, and continued circuit thrombosis despite heparin monitoring within therapeutic range during ECMO.
Balance of benefits versus harms:Although these studies may suggest use of bivalirudin during pediatric ECMO is safe, the optimal use, dosing adjustment algorithms, or role as a superior agent to heparin requires multicenter investigation using standardized definitions of bleeding and thrombosis and control of other potentially confounding factors. As such, there is insufficient evidence to recommend using bivalirudin as an initial anticoagulant for pediatric patients. Some pediatric centers are, however, using bivalirudin as the initial anticoagulant on ECMO, but widespread acceptance and agreement for this practice are not established.
Other evidence to decision considerations:Important considerations when using bivalirudin include concern for the risk of bleeding in certain postoperative patients. In addition, low-circuit flow states and/or regional stasis may induce thrombosis due to rapid local cleavage of bivalirudin that shortens the half-life of the drug (38). This phenomenon may be relevant when weaning ECMO flows or trialing off ECMO. Caution should also be exercised in patients with severe cardiac dysfunction who may have areas of stagnant blood within the heart. Some centers report preemptive heparin administration during low flow states or trials-off to minimize circuit thrombus formation. There is insufficient clinical information to make a recommendation about other DTIs.
Good Practice Statement2.4 In ECMO patients who develop heparin induced thrombocytopenia (HIT), all heparin should be discontinued, and direct thrombin inhibitors should be used for anticoagulation.93% agreement (n = 44), median 9, IQR 8–9.
Summary of the evidence:HIT is an immune-mediated adverse drug reaction caused by antibodies to complexes of platelet factor 4 and UFH. The risk of thrombosis (venous and arterial) is high and increased morbidity and mortality are reported in patients who develop HIT. In the pediatric population, cases of HIT have been increasingly reported, however, true incidence/prevalence is unclear as criteria for confirmation of HIT are not provided in every report (39). HIT can be challenging to diagnose in the critically ill pediatric population especially patients undergoing ECMO because one of the hallmarks in diagnosis, thrombocytopenia, is very common in critically ill children (40). Preliminary testing for HIT uses a heparin/platelet factor 4 antibody, with the serotonin-releasing assay providing confirmation in antibody-positive patients (41).
Balance of benefits versus harms:When the diagnosis of HIT is made, we suggest immediate cessation of heparin and transition to a DTI such as bivalirudin. Small case series using argatroban are also reported.
Adjunct Anticoagulant or Antiplatelet Medications Recommendation2.5 There is insufficient evidence in pediatric ECMO to recommend for or against the addition of alternate or adjunct anticoagulant or antiplatelet agents to UFH or direct thrombin inhibitors.Weak Recommendation, very low-quality pediatric evidence, 96% agreement (n = 46), median 8, IQR 7–9.
Summary of the evidence:There are no published prospective studies in critically ill children supported with ECMO comparing alternate or adjunct anticoagulant medication outside UFH or DTIs (Supplemental Table 2, https://links.lww.com/PCC/C495). The use of nafamostat mesilate (a synthetic serine protease inhibitor and short-acting anticoagulant) in addition to UFH was reported in a small series of newborns with hemorrhagic complications before or during ECMO (42). Using lower than standard UFH dosing and tolerating lower activated clotting time, bleeding was well controlled in 8 of the 12 neonates. As a single report with no comparison group, conclusions about the use of nafamostat mesilate are limited.
The use of adjunct anticoagulant medications has been reported in VAD patients. The first multi-institutional attempt to standardize anticoagulation therapy for pediatric extracorporeal support was the EXCOR Pediatric VAD Investigational Device Exemption study (43). Antithrombotic management was standardized using the Edmonton anticoagulation and platelet inhibition protocol. The goal of this study was to evaluate the safety and efficacy of the Berlin Heart EXCOR Pediatric VAD not to determine an optimal anticoagulation strategy. However, information about the addition of antithrombotic therapy and risk of bleeding and thrombosis has led to further revision of the anticoagulation and platelet inhibition strategy in this population (44). Centers have reported lower stroke rates with the addition of antiplatelet drugs and alternate dosing strategies to the Edmonton protocol. Although there are important differences between pediatric VAD and pediatric ECMO patients, additional studies focused on pediatric ECMO patients are needed and could build on lessons learned in the VAD population.
Other evidence to decision considerations:The use of adjunct anticoagulants or antiplatelet agents in adults and children with a hypercoagulable state supported with ECMO has been reported during the recent COVID-19 pandemic (45,46). Although there is little evidence to support or refute this practice in pediatric ECMO, use of such agents is standard practice in adults receiving cardiac stents or other procedures and has been reported in adult ECMO patients or anecdotal pediatric case reports (47). More specific evaluation of use of adjunct anticoagulants and antiplatelet agents in the pediatric ECMO population should be performed to establish efficacy or risk with these agents.
CONCLUSIONSClinical evidence to guide optimal anticoagulant medication selection in pediatric ECMO is sparse. Although strong consensus was reached on systemic anticoagulation during ECMO to prevent circuit and patient thrombosis, sufficient high-quality evidence is not available to recommend bivalirudin as a first-line anticoagulant or make a recommendation regarding adjunct anticoagulant or antiplatelet agents. Additional multicenter studies with scientifically rigorous designs are required to inform optimal anticoagulation strategies in pediatric ECMO.
ACKNOWLEDGMENTSWe thank all members of the Pediatric Extracorporeal Membrane Oxygenation Anticoagulation CollaborativE (PEACE) for their support, especially during the COVID-19 pandemic. The authors acknowledge the important contributions of Dr. M. Patricia Massicotte to the design and execution of the PEACE project. In addition, we thank AABB, the American Society of Extracorporeal Therapists, the American Pediatric Surgical Association, the Children’s Hospital Neonatal Consortium, the Collaborative Pediatric Critical Care Research Network, the European Society for Pediatric and Neonatal Intensive Care, the International Society of Blood Transfusion, Pediatric Cardiac Critical Care Consortium, Pediatric Cardiac Intensive Care Society, the Society for Critical Care Medicine (Pediatric Section and Clinical Pharmacy and Pharmacology Section) and the Society of Thoracic Surgeons.
REFERENCES 1. Dalton HJ, Reeder R, Garcia-Filion P, et al.; Eunice Kennedy Shriver National Institute of Child Health and Human Development Collaborative Pediatric Critical Care Research Network: Factors associated with bleeding and thrombosis in children receiving extracorporeal membrane oxygenation. Am J Respir Crit Care Med. 2017; 196:762–771 2. O’Halloran CP, Andren KG, Mecklosky J, et al.: Mortality and factors associated with hemorrhage during pediatric extracorporeal membrane oxygenation. Pediatr Crit Care Med. 2020; 21:75–81 3. Muszynski JA, Reeder RW, Hall MW, et al.; Eunice Kennedy Shriver National Institute of Child Health and Human Development Collaborative Pediatric Critical Care Research Network (CPCCRN): RBC transfusion practice in pediatric extracorporeal membrane oxygenation support. Crit Care Med. 2018; 46:e552–e559 4. Bembea MM, Annich G, Rycus P, et al.: Variability in anticoagulation management of patients on extracorporeal membrane oxygenation: An international survey. Pediatr Crit Care Med. 2013; 14:e77–e84 5. Ozment CP, Scott BL, Bembea MM, et al.: Anticoagulation and transfusion management during neonatal and pediatric extracorporeal membrane oxygenation: A survey of medical directors in the United States. Pediatr Crit Care Med. 2021; 22:530–541 6. Baird CW, Zurakowski D, Robinson B, et al.: Anticoagulation and pediatric extracorporeal membrane oxygenation: Impact of activated clotting time and heparin dose on survival. Ann Thorac Surg. 2007; 83:912–9; discussion 919 7. Bridges BC, Ranucci M, Lequier L: Anticoagulation and disorders of haemostasis. In: The ELSO Red Book. Fifth Edition. Brogan RV, Lequier L, Lorusso R, (Eds). Ann Arbor, MI, Extracorporeal Life Support Organization, 2017. p 831 8. Moynihan K, Johnson K, Straney L, et al.: Coagulation monitoring correlation with heparin dose in pediatric extracorporeal life support. Perfusion. 2017; 32:675–685 9. Weitz JI, Hudoba M, Massel D, et al.: Clot-bound thrombin is protected from inhibition by heparin-antithrombin III but is susceptible to inactivation by antithrombin III-independent inhibitors. J Clin Invest. 1990; 86:385–391 10. Buck ML: Bivalirudin as an alternative to heparin for anticoagulation in infants and children. J Pediatr Pharmacol Ther. 2015; 20:408–417 11. Alexander PMA, Bembea M, Cashen K, et al.; Pediatric Extracorporeal Membrane Oxygenation (ECMO) Anticoagulation CollaborativE (PEACE), in collaboration with the Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network, the Pediatric Critical Care Blood Research Network (BloodNet), and the Pediatric ECMO subgroup of PALISI and the Extracorporeal Life Support Organization (PediECMO): Executive summary: The Pediatric Extracorporeal Membrane Oxygenation Anticoagulation CollaborativE Consensus Conference. Pediatr Crit Care Med. 2024; 25:643-675 12. Hayden JA, van der Windt DA, Cartwright JL, et al.: Assessing bias in studies of prognostic factors. Ann Intern Med. 2013; 158:280–286 13. Higgins JPT, Sterne JAC, Savović J, et al.: A revised tool for assessing risk of bias in randomized trials In: Cochrane Methods. Chandler J, McKenzie J, Boutron I, et al (Eds). Cochrane Database of Systematic Reviews 2016; 10 (Suppl 1) 14. Sterne JAC, Savovic J, Page MJ, et al.: RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ. 2019; 366:l4898 15. Balshem H, Helfand M, Schunemann HJ, et al.: GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011; 64:401–406 16. Neumann I, Santesso N, Akl EA, et al.: A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016; 72:45–55 17. Alonso-Coello P, Oxman AD, Moberg J, et al.; GRADE Working Group: GRADE Evidence to Decision (EtD) frameworks: A systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016; 353:i2089 18. Alonso-Coello P, Schunemann HJ, Moberg J, et al.; GRADE Working Group: GRADE Evidence to Decision (EtD) frameworks: A systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016; 353:i2016 19. Neumann I, Brignardello-Petersen R, Wiercioch W, et al.: The GRADE evidence-to-decision framework: A report of its testing and application in 15 international guideline panels. Implement Sci. 2016; 11:93 20. Diamond IR, Grant RC, Feldman BM, et al.: Defining consensus: A systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol. 2014; 67:401–409 21. Fitch K, Bernstein SJ, Aguilar MD, et al.: The RAND/UCLA Appropriateness Method User’s Manual. Santa Monica, CA, RAND, 2001 22. Lamarche Y, Chow B, Bédard A, et al.: Thromboembolic events in patients on extracorporeal membrane oxygenation without anticoagulation. Innovations (Phila). 2010; 5:424–429 23. Chung YS, Cho DY, Sohn DS, et al.: Is stopping heparin safe in patients on extracorporeal membrane oxygenation treatment? ASAIO J. 2017; 63:32–36 24. Fina D, Matteucci M, Jiritano F, et al.: Extracorporeal membrane oxygenation without systemic anticoagulation: A case-series in challenging conditions. J Thorac Dis. 2020; 12:2113–2119 25. Wood KL, Ayers B, Gosev I, et al.: Venoarterial-extracorporeal membrane oxygenation without routine systemic anticoagulation decreases adverse events. Ann Thorac Surg. 2020; 109:1458–1466 26. Olson SR, Murphree CR, Zonies D, et al.: Thrombosis and bleeding in extracorporeal membrane oxygenation (ECMO) without anticoagulation: A systematic review. ASAIO J. 2021; 67:290–296 27. Whittlesey GC, Drucker DE, Salley SO, et al.: ECMO without heparin: Laboratory and clinical experience. J Pediatr Surg. 1991; 26:320–324; discussion 324 28. Bates A, Buchholz H, Freed D, et al.: Bivalirudin experience in a heterogeneous ventricular assist device population. ASAIO J. 2020; 66:677–682 29. VanderPluym CJ, Cantor RS, Machado D, et al.: Utilization and outcomes of children treated with direct thrombin inhibitors on paracorporeal ventricular assist device support. ASAIO J. 2020; 66:939–945 30. Ryerson LM, Balutis KR, Granoski DA, et al.: Prospective exploratory experience with bivalirudin anticoagulation in pediatric extracorporeal membrane oxygenation. Pediatr Crit Care Med. 2020; 21:975–985 31. Nagle EL, Dager WE, Duby JJ, et al.: Bivalirudin in pediatric patients maintained on extracorporeal life support. Pediatr Crit Care Med. 2013; 14:e182–e188 32. Machado DS, Garvan C, Philip J, et al.: Bivalirudin may reduce the need for red blood cell transfusion in pediatric cardiac patients on extracorporeal membrane oxygenation. ASAIO J. 2021; 67:688–696 33. Schill MR, Douds MT, Burns EL, et al.: Is anticoagulation with bivalirudin comparable to heparin for pediatric extracorporeal life support? Results from a high-volume center. Artif Organs. 2021; 45:15–21 34. Seelhammer TG, Bohman JK, Schulte PJ, et al.: Comparison of bivalirudin versus heparin for maintenance systemic anticoagulation during adult and pediatric extracorporeal membrane oxygenation. Crit Care Med. 2021; 49:1481–1492 35. Hamzah M, Jarden AM, Ezetendu C, et al.: Evaluation of bivalirudin as an alternative to heparin for systemic anticoagulation in pediatric extracorporeal membrane oxygenation. Pediatr Crit Care Med. 2020; 21:827–834 36. Campbell CT, Diaz L, Kelly B: Description of bivalirudin use for anticoagulation in pediatric patients on mechanical circulatory support. Ann Pharmacother. 2021; 55:59–64 37. Snyder CW, Goldenberg NA, Nguyen ATH, et al.: A perioperative bivalirudin anticoagulation protocol for neonates with congenital diaphragmatic hernia on extracorporeal membrane oxygenation. Thromb Res. 2020; 193:198–203 38. Ranucci M: Bivalirudin and post-cardiotomy ECMO: A word of caution. Crit Care. 2012; 16:427 39. Avila ML, Shah V, Brandao LR: Systematic review on heparin-induced thrombocytopenia in children: A call to action. J Thromb Haemost. 2013; 11:660–669 40. Avila L, Amiri N, Yenson P, et al.: Heparin-induced thrombocytopenia in a pediatric population: Implications for clinical probability scores and testing. J Pediatr. 2020; 226:167–172.e2 41. Thawani R, Nannapaneni S, Kumar V, et al.: Prediction of heparin induced thrombocytopenia (HIT) using a combination of 4Ts score and screening immune assays. Clin Appl Thromb Hemost. 2020; 26:1076029620962857 42. Nagaya M, Futamura M, Kato J, et al.: Application of a new anticoagulant (Nafamostat Mesilate) to control hemorrhagic complications during extracorporeal membrane oxygenation—a preliminary report. J Pediatr Surg. 1997; 32:531–535 43. Fraser CD Jr, Jaquiss RD, Rosenthal DN, et al.; Berlin Heart Study Investigators: Prospective trial of a pediatric ventricular assist device. N Engl J Med. 2012; 367:532–541 44. Rosenthal DN, Lancaster CA, McElhinney DB, et al.: Impact of a modified anti-thrombotic guideline on stroke in children supported with a pediatric ventricular assist device. J Heart Lung Transplant. 2017; 36:1250–1257 45. Smolarz A, McCarthy P, Shmookler A, et al.: Utilization of thromboelastogram and inflammatory markers in the management of hypercoagulable state in patients with COVID-19 requiring ECMO support. Case Rep Crit Care. 2021; 2021:8824531 46. Schneider J, Tilford B, Safa R, et al.: Extracorporeal membrane oxygenation for multisystem inflammatory syndrome in children. Perfusion. 2022; 37:639–642 47. Staudacher DL, Biever PM, Benk C, et al.: Dual antiplatelet therapy (DAPT) versus no antiplatelet therapy and incidence of major bleeding in patients on venoarterial extracorporeal membrane oxygenation. PLoS One. 2016; 11:e0159973
Comments (0)