
Remember me





We evaluated treatment and surgical site complications of infected mandibular fractures. Altogether 4.5% of patients with fracture in the dentate part of the mandible had a clinically infected fracture at the time of surgery in this single-centre study covering a time span of 11 years. Postoperative surgical site complications were common in this subset of patients, afflicting 31.7% of cases. Many of these occurred with a notable delay of up to four months, emphasizing the importance of postoperative follow-up. Infected fractures can be selectively treated intraorally, especially if the infection is mild, but due to the risk of wound dehiscence, careful patient selection is required. Clinicians most often chose the extraoral approach in severely infected fractures and in cases with major comminution. However, infection complications occur regardless of the approach. Nevertheless, severe postoperative infections and non-union are rare.
Patient compliance-related factors were the most notable cause for delayed surgery (73.2%). Substance and alcohol abuse was quite common in this patient population (46.3%), which might cause the lack of understanding of the consequences of injury and explain the delay in seeking treatment. In our previous study in the same department, substance and alcohol abuse was lower among mandibular fracture patients in general (23.4%) [3]. However, 19.5% had a previous assessment with a health care professional after the injury, but the fracture was not detected and became infected later. In recent studies, mandibular fractures were missed in 20% of patients aged over 60 years [15] and in 14.8% of children (< 20 years) [16] during patients’ first health care assessment. Fractures were missed more frequently in elderly patients who lived in nursing homes or were in hospital at the time of injury and in patients aged under 13 years. Thus, careful clinical examination and imaging examinations (dental panoramic radiograph and/or computed tomography) are strongly recommended for all patients with recent mandibular injury.
Surgical site healing may be affected by local circumstances in the fracture site, such as severity of infection, atrophic mandible, patient-related factors, and the surgeon’s experience and preferences. Additionally, a recent study showed that severe external wounds increase the incidence of overall complication and infections[17]. No patients in this study were edentulous; thus, the presence of teeth and occlusion may have contributed to infection. As presented in our results, the clinicians choose the approach and osteosynthesis technique according to the severity of infection and fracture comminution. Reconstruction plate with or without combined non-reconstruction plate was used in 19 patients (46.3%), and these patients had a complication rate of 31.6%. Ghanem et al. [12] investigated the use of 2.3 mm reconstruction bone plates in the treatment of unstable infected mandibular fractures in 32 patients, none of whom showed postoperative evidence of infection or hardware failure. However, in that study, the definition of primary infection was based on delay from injury, and clinical signs of infection were not considered. According to our results, infection complications cannot be completely prevented by reconstruction plate or extraoral approach in clinically infected fractures.
In addition to or even instead of the type of plate, attention should be paid to the length, type, and stability of screws, the accuracy of the reduction, tissue handling during surgery, and the effect of teeth and occlusion on fracture site healing. Thus, the results may be explained by several factors that should be considered in clinical work. Careful infection debridement, optimal fracture reduction, and support for treatment compliance are needed to prevent complications.
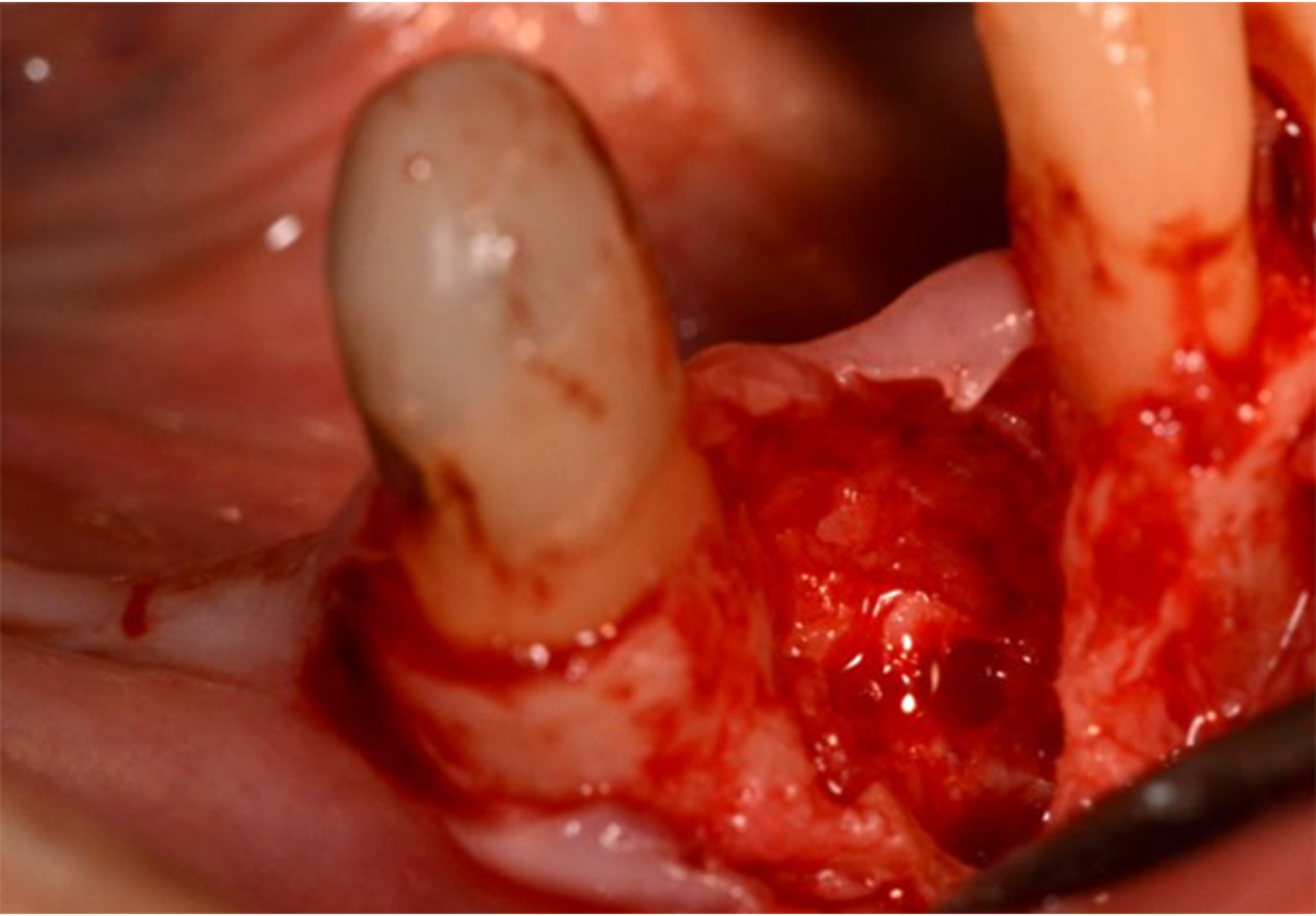
Only one patient received bone grafting in primary fracture surgery (Fig. 2). Benson et al. [13] studied bone grafts in the presence of pus and included 50 infected fractures. They reported that four patients developed recurrent infection, and three had non-union with loss of graft. The only correlating factor with failure was immunocompromising disease. Thus, immediate grafting in infected mandibular fractures seems effective. However, based on our data, surprisingly, mandibular fracture defects associated with infection healed without bone grafting, and non-union was a rare complication.
Fig. 2
a The patient was evaluated for an infected mandibular fracture two months after falling down stairs. A purulent wound formed in the lower jaw after falling, which was treated by medical doctors with two courses of antibiotics. Before ending up in the oral and maxillofacial emergency clinic, the patient also received a blow to her mandible. The patient had an infected symphysis fracture and a fracture in the left condyle. b The patient had osteolysis, fragmentation, and chronic infection in the fracture line in the symphysis that can be seen in the preoperative 3D reconstruction of computed tomography. The occlusion was surprisingly in place, but clinically the fracture fragments were mobile, and the symphysis fracture was found to be non-ossified. c A reconstruction plate was pre-bent on a 3D-printed model to ensure the comprehensive fit of the reconstruction plate on the lower border of the mandible. Because there were no changes in occlusion, preoperative virtual reduction of the fracture was not required. Extraoral approach was used for osteosynthesis. The reconstruction plate was first fixed in place and removed during careful local debridement of the fracture line. A free iliac crest bone graft was harvested and placed in the area of the mandibular bone defect. Right lower incisors were extracted during the surgery. Teeth that were close to the fracture line required endodontic treatment. Patient developed recurrent infection five weeks postoperatively, which, however, did not affect the ossification process. Patient’s (Fig. 2a) dental panoramic radiograph confirms a favorable recovery process 4.5 months postoperatively. Left condyle fracture healed without surgery
In infected mandibular fractures, antibiotic therapy is indicated and can be targeted more precisely after specimen culturing. In a previous study [7], alpha and beta-haemolytic streptococci were the most common pathogens found in cultures. Furthermore, viridans streptococci, especially Streptococcus anginosus, were the predominant bacteria cultured in our patient population. Empirical antibiotic treatment was started when the patient entered the hospital. Antibiotic treatment was in most cases targeted after the result of bacterial culture. The duration of postoperative antibiotic course varied between 2 and 33 days (mean 11.2 days, median 11 days) and is clearly longer than in mandibular fractures without clinical infection signs prior to surgery [3]. However, complications were not prevented by antibiotic medication or anticipated by anamnesis. Only one patient had type 1 diabetes and had no postoperative complications. Smoking or alcohol/drug abuse did not explain complication rates (Table 3). Future studies should focus on effective local care to prevent primary infection and avoid prolonged antibiotic therapies and recurrent infections.
Limitations of this study comprise its retrospective nature, lack of established protocol in the surgical approach and fixation method selection, and the rather small study population due to the low incidence of these types of fractures. Multicentre studies would provide more scientific evidence of optimal treatment for these patients. In addition, some patients were lost during follow-up, and thus, minor surgical site complications may have gone unrecorded in our data. However, as the department is the region’s only emergency department treating mandibular fractures, patients would have most likely made contact had notable complications occurred.
In conclusion, adequate and early diagnosis of mandibular fractures is essential to reduce the occurrence of infection complications. Both intraoral and extraoral approaches can be successfully used in infected mandibular fractures, but patient selection should be done with care and wound dehiscence risk related to intraoral approach noted. Infected mandibular fractures heal mainly without bone grafting, and non-union is a rare complication. Less severe surgical site complications are common and occur in almost one-third of patients, with a delay of up to three or four months, emphasizing the importance of postoperative follow-up. Because of low treatment compliance and high surgical site complication risk, comprehensive treatment in the primary phase is critical in this patient population.
Comments (0)