
Remember me

Anastomotic leak (AL) is a serious complication of colorectal surgery, with an incidence ranging from 3% to 19%.1–3 AL has a negative oncologic prognostic impact after rectal cancer resection, in addition to increased postoperative morbidity and mortality, prolonged hospital stays, and increased health care costs.2,4–8
Left-sided colorectal anastomoses exhibit higher AL rates compared to ileocolic anastomoses, with low colorectal anastomoses at especially high risk. Multiple risk factors have been identified for AL, including patient factors, such as nutritional status and neoadjuvant therapy, and operative factors, such as tissue perfusion and tension at the anastomotic site. Left-sided colorectal resections are at higher risk of requiring additional surgical mobilization compared to other colon resections to offset anastomotic tension. This can lead to disrupted vascular collateralization at the anastomotic site. Inadequate perfusion of perianastomotic tissue has been reported to be an important risk factor in AL pathophysiology.9,10 Accurately measuring tissue perfusion in real time thus represents a promising technique for decreasing the morbidity of left-sided colorectal surgery by decreasing the incidence of AL.
Advanced visualization and physiological imaging technologies have been developed to complement traditional methods of intraoperative assessment of anatomy and tissue perfusion, such as palpation of mesenteric vessels or visual inspection of tissue appearance with the naked eye.9,11–15 One technology with the potential to improve surgical outcomes is near-infrared indocyanine green (ICG) fluorescence angiography (ICG-FA).16 ICG-FA has gained increasing acceptance as a useful adjunct for real-time intraoperative tissue microperfusion assessment in open, laparoscopic, and robotic-assisted colorectal surgery.
The data around the benefit of ICG-FA in colon and rectal cases is mixed. ICG-FA has been shown to alter intraoperative clinical decision-making in 7.9% to 27.3% of colorectal surgery cases but does not always result in a difference in the incidence of AL.12,17–19 However, a meta-analysis by Arezzo et al16 demonstrated that the use of ICG-FA was associated with a reduction in AL in patients who underwent surgery for rectal cancer. The use of ICG-FA is limited by certain factors, such as pharmacokinetics of the ICG fluorophore, allergic and adverse reactions to the dye, variations in its use among surgeons, lack of standardization of signal interpretation, false-positive findings on repeat assessments, additional staff coordination required for use, and the need for costly equipment upgrades.17,20,21 False-positive perfusion can be seen with ICG when blood flow stops and blood is stagnant; because the dye is previously present, it suggests positive perfusion in tissue despite the absence of any active flow. Capillary leakage, dye retention in interstitial tissues, and subjective visual assessment increase the likelihood of false-positive ICG interpretation.22,23 Given the heterogenous literature on ICG-FA efficacy in reducing AL rate, consideration should be given to alternative technologies to aid surgical perfusion visualization.
Another technology with much promise for real-time physiological imaging is laser speckle contrast imaging (LSCI).24,25 LSCI measures microvascular tissue perfusion using a dynamic interference pattern produced when a coherent laser light illuminates red blood cells.26 This can be performed in real time without injection of a fluorophore contrast dye and produces accurate and repeatable assessments unaffected by previous evaluations.
We hypothesized that LSCI would effectively demonstrate real-time, repeatable tissue perfusion information and inform surgeons’ intraoperative decision-making around tissue resection and colorectal anastomosis. Furthermore, we aimed to test whether post hoc quantification of LSCI data using relative perfusion unit (RPU) analysis could provide robust, repeatable, and comparable perfusion quantification and reveal precise ischemic patterns around the colonic watershed zone and perianastomotic tissues.
MATERIALS AND METHODS Setting and Patient SelectionThis study was conducted within the colorectal surgery division at a single tertiary referral academic institution. The study protocol was reviewed and approved by the entire Institutional Review Board (protocol ID: 2021H218). Adult patients (older than 18 years) undergoing elective left colocolonic or colorectal anastomoses (after left hemicolectomy, sigmoidectomy, or low anterior resection) via laparoscopic or robotic-assisted approach were eligible for enrollment in the intervention group. Patients were ineligible for enrollment if they were pregnant, lactating, or had a known allergy or history of adverse reaction to iodides or ICG. Patients were approached for participation, and informed consent was obtained for every enrolled patient before the day of surgery. Adverse events were explicitly monitored. Interim analysis was performed with the principal investigator, who found no safety concerns to halt the study.
This study aimed to recruit 40 patients, based on a power calculation from prior preclinical LSCI studies demonstrating 3 to 4 cm difference in ischemic line of demarcation (LOD) between white light imaging (WLI) and LSCI in a blinded survey of 21 surgeons.23 These results were extrapolated to clinical use, hypothesizing that LSCI could indicate different LODs in a clinical trial of a similar sample size.27 This study was not powered to detect differences in clinical outcomes like ALs or surgical decision-making.
For analysis, a case-matched retrospective cohort was composed of all left-sided colorectal surgeries performed the year before the study, including patients who would have been eligible for the study. The retrospective cohort was not matched on specific cases, and ICG was not routinely performed in these cases.
TechnologyThe device used for this study, the ActivSight imaging module (Activ Surgical, Boston, MA), is FDA-510(k) cleared for endoscopic fluorescence and near-infrared imaging in minimally invasive surgery. ActivSight enables surgeons to visually assess tissue perfusion using both LSCI and ICG-FA and to visualize extrahepatic biliary structures using ICG fluorescence. The ActivSight imaging module, which fits between a standard laparoscope and camera, allows for imaging of near-infrared light (LSCI and ICG) using an infrared sensor combined with standard RGB video. Images from the white light camera and the infrared sensor are combined to create a real-time overlay of either the LSCI perfusion colormap or ICG fluorescence on the white light camera image. The safety and feasibility of ActivSight have previously been published.28
Intraoperative Perfusion AssessmentPerfusion assessment of the colon and rectum was performed intraoperatively in real time by the surgeon using WLI, ICG-FA, and LSCI. For laparoscopic surgeries, a standard laparoscope with an ActivSight imaging module was used throughout the case. For robotic surgeries, an ancillary laparoscope with the ActivSight imaging module was inserted through preexisting robotic assist port sites for tissue perfusion assessment only.
Perfusion assessment was performed at 3 standardized time points for each surgery:
T1: Assessment of the ischemic LOD after colonic devascularization and distal division of the colorectal segment to be removed but before proximal transection of the specimen. Surgeons indicated where they perceived the line demarcating well-perfused vs ischemic tissue to be located at this time using all 3 visualization modes (WLI, ICG-FA, and LSCI). WLI LOD was assessed before viewing any advanced visualization data to prevent anchoring bias. T2: Assessment of the proximal and distal tissue serosal/adventitial surfaces to be anastomosed before anastomosis. T3: Assessment of the anastomosis after completion.Two milligrams of ICG was injected intravenously and interpreted within 1 to 3 minutes at T1 to enable ICG-FA assessment of the ischemic LOD following published best practices.29 Repeat ICG injections at T2 and T3 were left to the surgeon discretion.
Postoperative Surgeon SurveyImmediately after each case, surgeons were interviewed with a standardized questionnaire to assess the usability of the device, their interpretation of the advanced visualization information, and any influence it had on their clinical decision-making.
Post Hoc RPU Analysis of LSCI DataLSCI data from the 3 time points were analyzed using RPU analysis. This methodology converts raw LSCI data, which can differ in absolute value due to technical, equipment, patient, and tissue factors, into a relative scale. RPU quantifies LSCI perfusion for a target tissue as a percentage relative to maximally perfused vs ischemic tissue. To determine RPU, a reference area of maximum perfusion “hot” (a surface-level capillary on the tissue of interest) is selected and RPU for target tissue “target” is calculated as “target”/“hot,” yielding an RPU percentage on a range from 0% (no flow/perfusion) to 100% (“hot”). This type of relative perfusion analysis is similar to those performed for relative perfusion analysis of ICG-FA.30 RPU values allow for pooled analysis of each time point used in this study to compare the magnitude and distribution of tissue ischemia more precisely.
Statistical AnalysisStatistical analyses were performed using Microsoft Excel. The Student t test was used to compare continuous variables, and the Fisher exact probability test was used to compare categorical variables. The threshold for statistical significance (α) was set at 0.05.
RESULTSSeven board-certified colorectal surgeons participated in this study, with a mean practice history of 9 years (range, 3–17). Forty consecutive patients were enrolled in the intervention group from March 2022 to March 2023. The case-matched retrospective cohort included 83 patients.
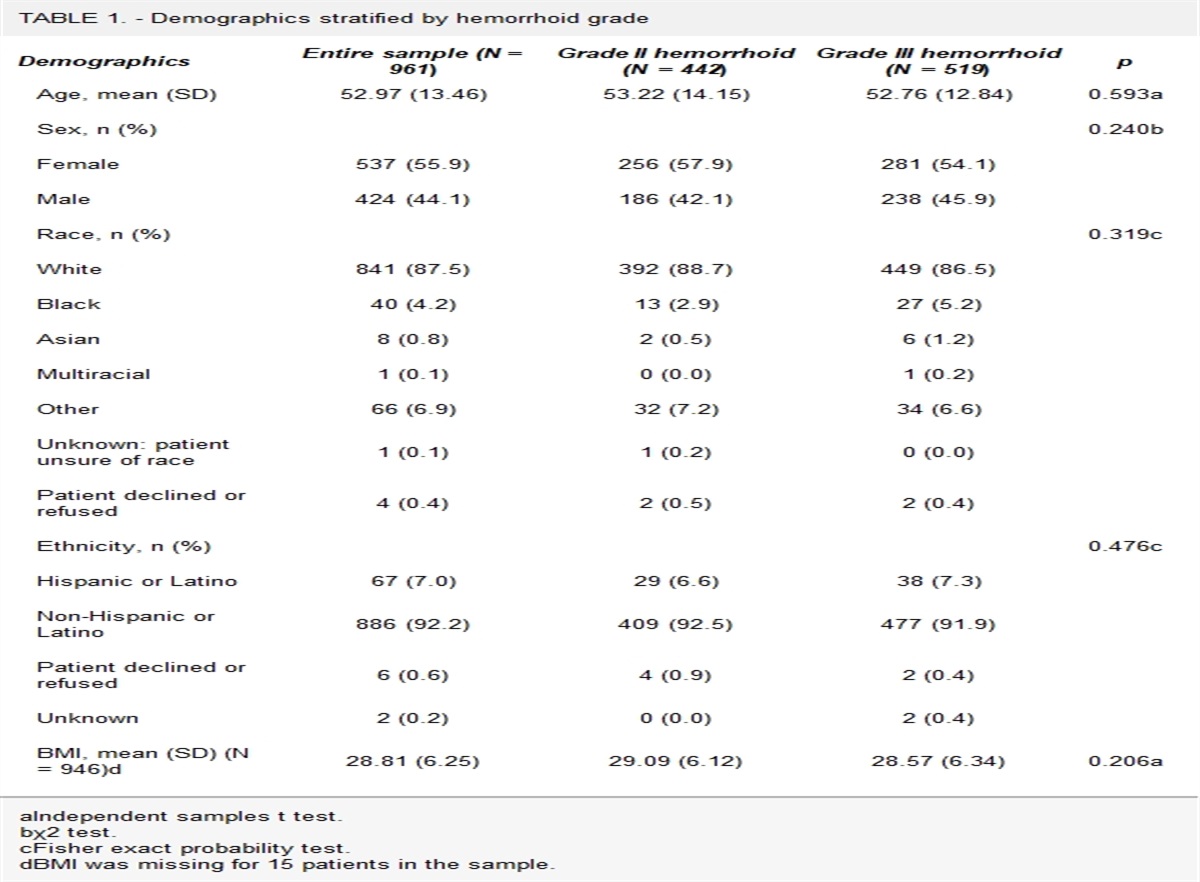
Study patients were similar to the case-matched retrospective cohort from the same institution with respect to BMI, race, and sex but were slightly older (62.3 vs 56.1 years old, p = 0.012; Table 1). Although this study was not powered to detect a difference, the colorectal AL rate of the study population (1/40) was similar to that recorded in the retrospective cohort (3/83; Table 1), which is lower than the national average.2 ALs were diagnosed on the basis of clinical suspicion for leak with radiologic confirmation, in concordance with standard clinical practice at the study institution. The diversion rate was 32.5% (13/40). Case duration and operating room time were not different between the study cases and the retrospective cohort (Table 1).
TABLE 1. - Comparison of study patient population and case-matched retrospective population Patient demographics Retrospective (n = 83) Study (n = 40) p Age, y, mean 56.1 63 0.008* BMI, mean 29.8 28.1 0.126 Sex, n (%) 0.037* Male 37 (45%) 26 (65%) Female 46 (55%) 14 (35%) Race 1.000 White 70 (84%) 34 (85%) Non-White 13 (16%) 6 (15%) Indication 0.340 Cancer 44 (53%) 25 (63%) Benign 39 (47%) 15 (37%) No. of comorbidities 0.065 0–2 77 (93%) 32 (80%) 3+ 6 (7%) 8 (20%) Case duration, mean Robotic LAR 5:49 (n = 17) 6:42 (n = 8) 0.314 Laparoscopic LAR 4:22 (n = 19) 3:58 (n = 9) 0.585 Robotic sigmoid 3:58 (n = 12) 4:13 (n = 3) 0.797 Laparoscopic sigmoid 3:01 (n = 18) 3:35 (n = 13) 0.070 Laparoscopic left 3:33 (n = 5) 3:20 (n = 4) 0.635 Leak rate, n (%) 1.000 No leak 80 (96.4%) 39 (97.4%) Leak 3 (3.6%) 1 (2.6%)Continuous variable p values are calculated with the t test and categorical variables with the Fisher exact probability test.
LAR = low anterior resection.
*Statistically different.
Twenty-three of 40 cases were analyzed for LOD concordance between ICG-FA and LSCI and 21 of 40 cases for LOD concordance between WLI and LSCI at the T1 time point. Data from 2 cases were not available for analysis because of corrupted video data, and the remaining videos did not have frames sufficient for determination. It should be noted that both analyses meet the predetermined threshold of 21 cases needed to distinguish significant differences between LSCI/ICG-FA and WLI.23
LSCI and ICG-FA indicated the same LOD in 83% (19/23) of cases and did not have statistically different levels of discordance with an average absolute delta distance of 0.63 cm (p = 0.16). LSCI indicated a more proximal LOD in 3 of the 4 cases with ICG-FA and LSCI discordance—perfusion did not appear to extend as distally toward the resection specimen with LSCI as with ICG-FA.
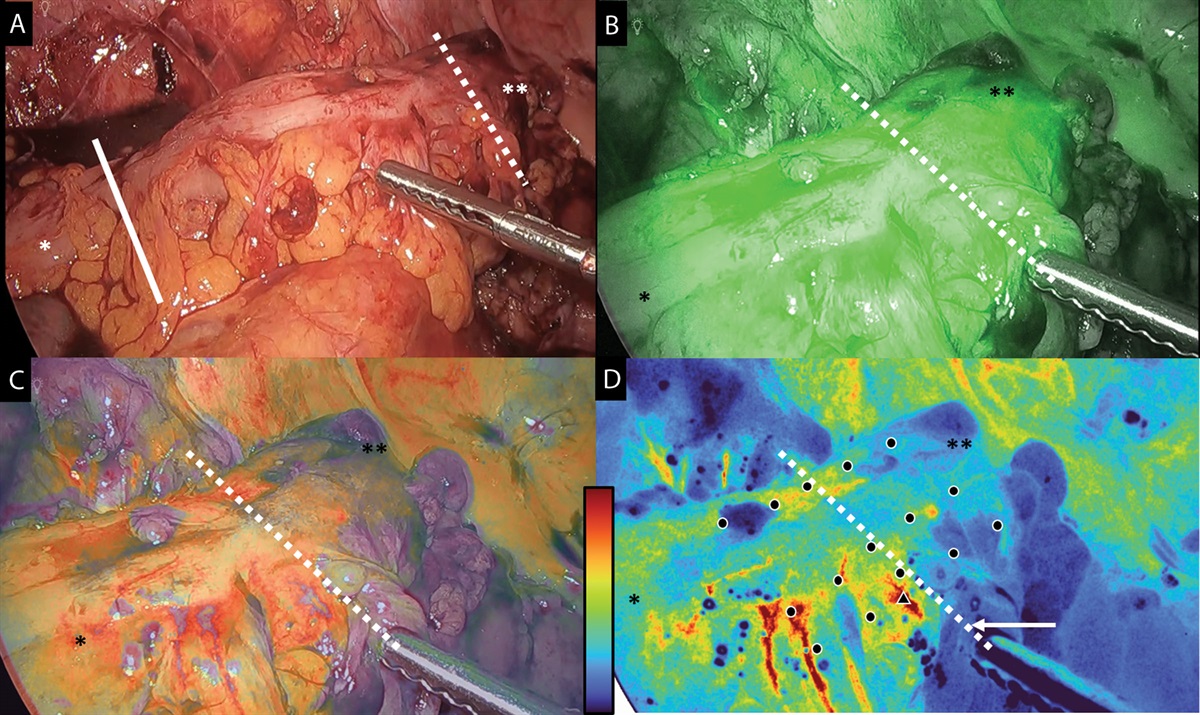
Figure 1 demonstrates an example of LOD as determined by the surgeon under WLI and advanced visualization methods (both LSCI and ICG-FA) at time point T1, with a solid line indicating where the surgeon interpreted the ischemic LOD to be using WLI only and dashed lines indicating the ischemic LOD using advanced visualization (ICG and LSCI). The magnitude of discordance between LOD indicated in WLI compared to LSCI and ICG was not statistically different when surgeons with ≥10 years of experience (3 surgeons) were compared to those with <10 years (4 surgeons; p = 0.50, p = 0.67).
 FIGURE 1.:
FIGURE 1.: Perfusion assessment of colonic ischemic LOD after devascularization. The single asterisk (*) represents the proximal colon and the double asterisks (**) represent the distal colon. The solid line indicates the surgeon real-time indication of LOD in WLI. Dashed lines represent the surgeon real-time indication of LOD with advanced imaging using LSCI and ICG-FA. The demarcation zone is shown in WLI (A), ICG-FA (B), and LSCI (C), in which perfusion is represented as a heat map, with higher perfusion using warm colors (red, orange, and yellow) and lower perfusion using cold colors (green and blue). D, Raw LSCI regions of interest data are converted to relative perfusion units. ICG-FA = and indocyanine green fluorescence angiography; LOD = line of demarcation; LSCI = laser speckle contrast imaging; WLI = white light imaging.
Surgeons reported that advanced visualization with LSCI and ICG-FA influenced intraoperative surgical decision-making in 7 of 40 cases (17.5%). In each of these cases, the change in clinical decision-making occurred after T1 when the surgeon chose where to make the proximal specimen transection, in part based on the determination of the ischemic LOD. No anastomotic revisions or other decision-making changes were performed after perfusion assessment at T2 and T3. In cases in which surgeons changed their decision-making, 5 videos were available for LOD discordance analysis. The remaining videos could not be analyzed because of corrupted video data or case flow factors, causing the surgeon not to mark an LOD intraoperatively in both WLI and LSCI. The average discordance between the ischemic LOD in WLI and LSCI was an absolute difference of 3.7 cm, compared to a difference of 0.23 cm (n = 21, p = 0.008) for cases without decision changes. LSCI resulted in discordant LODs both proximal and distal to the WLI-indicated LOD, depending on the case (Fig. 2). It was unclear what factors led to a more proximal or distal LOD using LSCI compared to WLI. In some cases, LSCI may help surgeons limit their colonic resections and preserve length for low anastomoses. Figure 2 presents a histogram of discordances between WLI and LSCI, highlighting cases in which surgeons changed decision-making (indicated by red boxes).
 FIGURE 2.:
FIGURE 2.: Histogram of the absolute distance discordance of the surgeon-indicated LOD using LSCI versus WLI (n = 21). Negative values indicate that the LSCI LOD is more proximal to the WLI LOD, and positive values indicate that the LSCI LOD is more distal to WLI LOD. Red bars indicate cases in which advanced visualization changed intraoperative clinical decision-making (n = 5), with an average absolute discordance of 3.7 cm, compared to 0.23 cm (p = 0.008) for cases without decision changes (n = 16). LOD = line of demarcation; LSCI = laser speckle contrast imaging; WLI = white light imaging.
Relative Tissue Perfusion AnalysisRPU analysis was performed at each time point to quantify, compare, and pool LSCI data. The RPUs at T1 are plotted in Figure 3 as a function of distance from the LOD identified by the surgeon intraoperatively on the LSCI color heat map (n = 30). Ten videos could not be analyzed because of corrupted video data, technical factors causing LSCI data to be too poor in quality for use in RPU analysis, or case flow factors causing the surgeon not to mark an LOD intraoperatively. The most proximal LSCI RPU measurement (–20 mm) was on average 8.31% higher than the RPU measurement at the surgeon-indicated LOD (p = 0.028), and the most distal measurement (+20 mm) was on average 19.40% lower (p = 2.04E–05). RPU analysis indicated a continuous gradient of perfusion that declines from perfused tissue (proximal) to devascularized tissue (distal) along the colonic watershed zone.
 FIGURE 3.:
FIGURE 3.: Average RPU are reported as a function of distance from the surgeon-indicated ischemic LOD (0 mm) with positive distance values indicating distal and negative distance values indicating proximal (n = 30). Twenty centimeters proximal to the LOD (*) is, on average, 8.31% higher than the surgeon-indicated LOD (p = 0.028), and 20 cm distal (**) is, on average, 19.40% lower (p = 2.04E–05). Plateaus of proximal (66%) and distal sides (40%) of the LOD are shown as dashed lines by calculating the average of the 3 most outer points (–20, –15, –10 and 10, 15, 20 cm). LOD = line of demarcation; RPU = relative perfusion unit.
At T2 time point, surgeons performed similar perfusion assessments in WLI, ICG-FA, and LSCI. Surgeons were asked to provide feedback on their perception of tissue perfusion, but no post hoc analysis was performed at this time point. At T3 time point of the study, when surgeons performed a perfusion assessment of the completed colorectal anastomosis in all visualization modalities (WLI, ICG-FA, and LSCI; Fig. 4), both advanced visualization modes (LSCI and ICG-FA) demonstrated relative ischemia at the anastomotic staple line intraoperatively.
 FIGURE 4.:
FIGURE 4.: Perfusion assessment of colorectal anastomosis. The single asterisk (*) represents the colon and the double asterisks (**) represent the rectum. The arrows indicates colorectal anastomosis, which is shown in standard white light (A), with indocyanine green fluorescence angiography (B), and LSCI (C) in which perfusion is represented as a heat map with higher perfusion as warm colors (red, orange, and yellow) and lower as cold colors (green and blue). D, Raw LSCI regions of interest data are converted to relative perfusion units. LSCI = laser speckle contrast imaging.
The RPUs at T3 are plotted in Figure 5 (n = 35). Five cases could not be analyzed because of corrupted video data or the inability to visualize the necessary tissue in the video data. The distribution of ischemia around the colorectal anastomoses at T3 is shown in this graph. The most proximal measurement (–20 mm) is an average of 35.31% higher than the anastomosis (p = 5.18E–16), and the most distal measurement (+20 mm) is an average of 25.98% higher (p = 6.29E–05). RPU quantifies relative ischemia at the anastomotic staple line compared to proximal and distal tissues.
 FIGURE 5.:
FIGURE 5.: Average RPUs are reported as a function of distance from the colorectal anastomosis (0 mm) with positive distance values indicating distal (rectal) and negative distance values indicating proximal (colonic; n = 35). Twenty centimeters proximal to the anastomosis (*) is on average 35.31% higher than the anastomosis (p = 5.18E–16), and 20 cm distal (**) is on average 25.98% higher (p = 6.29E–05). Plateaus of the colonic (65%) and rectal sides (57%) of the anastomosis are shown as dashed lines by calculating the average of the 3 most outer points (–20, –15, –10 and 10, 15, 20 cm). RPU = relative perfusion unit.
DISCUSSIONThis study investigated and compared the intraoperative utility of ICG-FA and novel LSCI available on a single technology platform to determine tissue perfusion vs ischemia in left-sided colorectal resection and anastomosis. In addition, post hoc quantification analysis was performed to more objectively analyze ischemic patterns using the raw infrared signals beyond what could be interpreted by naked eye heat map interpretation.
In 17.5% of cases in this study, surgeons changed an intraoperative decision based on information provided by advanced visualization. This is higher than in previous studies using ICG-FA alone, such as the 8% observed in the Pillar II trial.12 Although the majority of cases did not show a difference in perceived perfusion by white light or advanced imaging, in nearly 1 in 5 cases, surgeons appreciated a perfusion difference, with a LOD change up to 5.5 cm at the T1 measurement. An intraoperative decision to change the resection point was correlated to the magnitude of the difference demonstrated by enhanced visualization compared to white light. These results suggest that real-time intraoperative advanced visualization may add value to traditional inspection with the naked eye and WLI.1–3,17
The study was not intended to discern AL rates with or without advanced visualization, but there was a low leak rate (n = 1), which was statistically similar to the historical cohort. Notably, in the singular case resulting in AL in this study, the surgeon did not perceive any tissue ischemia when examining the anastomosis in WLI and advanced visualization (ICG-FA and LSCI). In addition, post hoc RPU analysis did not identify significant colonic perfusion differences before or after anastomosis creation. The leak was detected on postoperative day 14 and managed nonoperatively. These observations suggest that ischemia, at least at the time of the anastomosis, was not responsible for this AL.
Introducing new technology raises concerns regarding intraoperative workflow and efficiency. Although ICG-FA use and adoption have been more selective, the use of the advanced visualization module with ICG-FA and LSCI did not increase operative duration compared to the historical control cohort, suggesting that the technology could be incorporated easily into the surgical workflow. This may be driven by the fact that this is a visualization technology, which does not require contrast dye injection and timing when using LSCI.
Post hoc RPU analysis allows for more precise and objective perfusion assessment based on raw infrared signals placed along a standardized scale. The average ischemic demarcation based on RPU analysis was 1 cm more distal than the surgeon-indicated LOD based on their interpretation of the intraoperative LSCI heat map as indicated by the relative trough of RPU values 1 cm distal to the surgeon-indicated LOD (Fig. 3). RPU analysis precisely showed higher values on either side of a relatively ischemic anastomosis: blood flow at the level of the staple line of a colorectal anastomosis was lower than that in immediately surrounding tissues. This supports the role of collateral perfusion from proximal and distal tissues in anastomotic healing. When paired with capability of LSCI for repeated intraoperative assessments of perfusion without increased patient risk (eg, contrast load) or decreased fidelity (eg, contrast retention), RPU analysis may present a promising avenue for investigating anastomoses and anastomotic complications. Because advancements in computer vision may be useful in interpreting intraoperative information,31 more work is in the process to determine clinical correlations and implications of the RPU technology.
This study was powered to investigate technological and interpretive differences in intraoperative perfusion assessment between advanced ICG-FA and LSCI visualization technologies, similar to preclinical LSCI studies.23 Limitations of this study include low power with respect to detecting differences in AL rates and the fact that it was a single institution study. Randomization was not performed in this study, and cohort comparison to the intervention group relied on retrospective case-matching. Although ICG was injected uniformly at T1 and perfusion immediately assessed in 1 to 3 minutes, corresponding with best practices,29 repeat ICG injections at T2 and T3 were encouraged but ultimately left to surgeon discretion because of variation in surgeon preference of repeated ICG usage and patient safety. Therefore, ICG-FA perfusion assessment at T2 and T3 was not standardized. Due to the lack of ICG standardization at time points T2 and T3, ICG was only considered in LOD determination at time point 1, and time points T2 and T3 focused on LSCI RPU analysis alone to ensure that any differences in ICG protocol at time points T2 and T3 did not affect study outcomes. Extracorporeal vs intracorporeal anastomotic technique was also left to the surgeon discretion, which resulted in both extracorporeal and intracorporeal perfusion visualization that may have affected both LSCI and ICG-FA margin assessment across cases. LSCI perfusion assessment is affected by variables such as camera distance/angulation, tissue motion, and penetration depth.25 Therefore, another limitation in this study was the inability to standardize LSCI camera distance to target tissue because spatial distance in laparoscopic surgery is not easily determined. RPU analysis helps mitigate this limitation by quantifying perfusion values relative to other tissues in the same video frame. The use of advanced visualization (LSCI or ICG-FA) resulted in a rate of surgical decision change in this study of 17.5%, which is within the range of previously published studies of ICG, such as the PILLAR II trial (7.9% of cases) and data from the EURO-FIGS registry, which showed a decision change of 27.3%.12,18 We acknowledge there may have been a Hawthorne effect on practicing surgeons using a novel technology/device (LSCI) that could have increased the rate of decision changes.
CONCLUSIONThis study builds on previous literature suggesting that perfusion assessment during colorectal surgery is influential to the surgeon’s intraoperative decision-making, especially as it pertains to anastomotic creation. Perfusion assessment by LSCI was clinically similar to ICG-FA assessment without the drawbacks of fluorophore injection. An increasing discordance between perfusion assessment under WLI and LSCI is more likely to impact intraoperative surgical decision-making. Finally, this study demonstrated the feasibility and highly precise perfusion information obtained from relative perfusion analysis of LSCI data.
ACKNOWLEDGMENTSChandler Lowe, Clinical Research Coordinator, and Kayla Diaz, Clinical Research Manager, worked hard to help recruit and collect clinical data throughout the study.
REFERENCES 1. Guillou PJ, Quirke P, Thorpe H, et al.; MRC CLASICC trial group. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre, randomised controlled trial. Lancet. 2005;365:1718–1726. 2. Kang CY, Halabi WJ, Chaudhry OO, et al. Risk factors for anastomotic leakage after anterior resection for rectal cancer. JAMA Surg. 2013;148:65–71. 3. Stamos MJ, Brady MT. Anastomotic leak: are we closer to eliminating its occurrence? Ann Laparosc Endosc Surg. 2018;3:66. 4. Buchs NC, Gervaz P, Secic M, Bucher P, Mugnier-Konrad B, Morel P. Incidence, consequences, and risk factors for anastomotic dehiscence after colorectal surgery: a prospective monocentric study. Int J Colorectal Dis. 2008;23:265–270. 5. Lee SW, Gregory D, Cool CL. Clinical and economic burden of colorectal and bariatric anastomotic leaks. Surg Endosc. 2020;34:4374–4381. 6. Hammond J, Lim S, Wan Y, Gao X, Patkar A. The burden of gastrointestinal anastomotic leaks: an evaluation of clinical and economic outcomes. J Gastrointest Surg. 2014;18:1176–1185. 7. Mirnezami A, Mirnezami R, Chandrakumaran K, Sasapu K, Sagar P, Finan P. Increased local recurrence and reduced survival from colorectal cancer following anastomotic leak: systematic review and meta-analysis. Ann Surg. 2011;253:890–899. 8. Kulu Y, Tarantio I, Warschkow R, et al. Anastomotic leakage is associated with impaired overall and disease-free survival after curative rectal cancer resection: a propensity score analysis. Ann Surg Oncol. 2015;22:2059–2067. 9. Vignali A, Gianotti L, Braga M, Radaelli G, Malvezzi L, Di Carlo V. Altered microperfusion at the rectal stump is predictive for rectal anastomotic leak. Dis Colon Rectum. 2000;43:76–82. 10. Zarnescu EC, Zarnescu NO, Costea R. Updates of risk factors for anastomotic leakage after colorectal surgery. Diagnostics (Basel). 2021;11:2382. 11. Karliczek A, Benaron DA, Baas PC, Zeebregts CJ, Wiggers T, van Dam GM. Intraoperative assessment of microperfusion with visible light spectroscopy for prediction of anastomotic leakage in colorectal anastomoses. Colorectal Dis. 2010;12:1018–1025. 12. Jafari MD, Wexner SD, Martz JE, et al. Perfusion assessment in laparoscopic left-sided/anterior resection (PILLAR II): a multi-institutional study. J Am Coll Surg. 2015;220:82–92.e1. 13. Clancy NT, Soares AS, Bano S, Lovat LB, Chand M, Stoyanov D. Intraoperative colon perfusion assessment using multispectral imaging. Biomed Opt Express. 2021;12:7556–7567. 14. Mehdorn M, Köhler H, Rabe SM, et al. Hyperspectral imaging (HSI) in acute mesenteric ischemia to detect intestinal perfusion deficits. J Surg Res. 2020;254:7–15. 15. Briers JD. Laser Doppler, speckle and related techniques for blood perfusion mapping and imaging. Physiol Meas. 2001;22:R35–R66. 16. Arezzo A, Bonino MA, Ris F, et al. Intraoperative use of fluorescence with indocyanine green reduces anastomotic leak rates in rectal cancer surgery: an individual participant data analysis. Surg Endosc. 2020;34:4281–4290. 17. Jafari MD, Pigazzi A, McLemore EC, et al. Perfusion assessment in left-sided/low anterior resection (PILLAR III): a randomized, controlled, parallel, multicenter study assessing perfusion outcomes with PINPOINT near-infrared fluorescence imaging in low anterior resection. Dis Colon Rectum. 2021;64:995–1002. 18. Spota A, Al-Taher M, Felli E, et al. Fluorescence-based bowel anastomosis perfusion evaluation: results from the IHU-IRCAD-EAES EURO-FIGS registry. Surg Endosc. 2021;35:7142–7153. 19. Watanabe J, Takemasa I, Kotake M, et al. Blood perfusion assessment by indocyanine green fluorescence imaging for minimally invasive rectal cancer surgery (EssentiAL trial): a randomized clinical trial. Ann Surg. 2023;278. 20. Cassinotti E, Boni L, Della Porta M, Baldari L. The role of indocyanine green performing a minimally invasive right colectomy. Ann Laparosc Endosc Surg. 2021;6:30–30. 21. Towle EL, Richards LM, Kazmi SMS, Fox DJ, Dunn AK. Comparison of indocyanine green angiography and laser speckle contrast imaging for the assessment of vasculature perfusion. Neurosurgery. 2012;71:1023–1030. 22. Duprée A, Rieß H, Detter C, Debus ES, Wipper SH. Utilization of indocynanine green fluorescent imaging (ICG-FI) for the assessment of microperfusion in vascular medicine. Innov Surg Sci. 2018;3:193–201. 23. Nwaiwu CA, Buharin VE, Mach A, et al. Feasibility and comparison of laparoscopic laser speckle contrast imaging to near-infrared display of indocyanine green in intraoperative tissue blood flow/tissue perfusion and extrahepatic bile ducts in preclinical porcine models. J Am Coll Surg. 2021;233:S78–S79. 24. Kojima S, Sakamoto T, Nagai Y, Matsui Y, Nambu K, Masamune K. Laser speckle contrast imaging for intraoperative quantitative assessment of intestinal blood perfusion during colorectal surgery: a prospective pilot study. Surg Innov. 2019;26:293–301. 25. Heeman W, Steenbergen W, van Dam G, Boerma EC. Clinical applications of laser speckle contrast imaging: a review. J Biomed Opt. 2019;24:1–11. 26. Draijer M, Hondebrink E, van Leeuwen T, Steenbergen W. Review of laser speckle contrast techniques for visualizing tissue perfusion. Lasers Med Sci. 2009;24:639–651. 27. Bagiella E, Chang H. Power analysis and sample size calculation. J Mol Cell Cardiol. 2019;133:214–216. 28. Shah SK, Nwaiwu CA, Agarwal A, et al. First-in-human (FIH) safety, feasibility, and usability trial of a laparoscopic imaging device using laser speckle contrast imaging (LSCI) visualizing real-time tissue perfusion and blood flow without fluorophore in colorectal and bariatric patients. J Am Coll Surg. 2021;233:S45–S46. 29. Garoufalia Z, Wexner SD. Indocyanine green fluorescence guided surgery in colorectal surgery. J Clin Med. 2023;12:494. 30. Goncalves LN, van den Hoven P, van Schaik J, et al. Perfusion parameters in near-infrared fluorescence imaging with indocyanine green: a systematic review of the literature. Life (Basel). 2021;11:433. 31. Mascagni P, Alapatt D, Sestini L, et al. Computer vision in surgery: from potential to clinical value. NPJ Digit Med. 2022;5:163.
Comments (0)