Ralstonia species are non-fermented Gram-negative bacillus which can cause a variety of infections and even outbreaks in hospitals [4, 19]. The Ralstonia pickettii, R. mannitolilytica and R. insidiosa have been reported to be the most common clinically pathogenic pathogens with mis-dentification in clinical laboratory [13]. In our study, only 34 of the 48 clinical strains identified to be Ralstonia pickettii with VITEK 2 system were confirmed by the 16 S rDNA method, with an accuracy of only 70.83%. This indicates that the identification results of Ralstonia pickettii by conventional methods are not wholly reliable and should be confirmed with molecular assays.
Tom Coenye et al. performed a PCR experiment to identify Ralstonia pickettii, R. mannitolilytica and R. insidiosa using designed primers Rp-F1/Rp-R1, Rm-F1/Rm-R1 and Rp-F1/R38-R1 [13, 16]. It showed that there were corresponding target bands after the amplification of Ralstonia pickettii and R. mannitolilytica with common primers. Due to the crossing between primers in the identification of Ralstonia pickettii and R. insidiosa, two target bands showed up in R. insidiosa. Our results were complied with that of Tom Coenye’s [15, 16]. Michael P Ryan’s [20] also got the same results. In addition, the 16 S rDNA method was also conducted as a standard method to evaluate the accuracy of the PCR assays. The sensitivity and specificity of the PCR assays about Ralstonia pickettii, R. mannitolilytica and R. insidiosa were 85.3% and 85.7%, 100% and 100%, 71.4% and 90.2%, respectively. In comparison with the previous studies, the sensitivity and specificity are not significantly increase. This is considered to correlate with the types of bacteria selected to evaluate the accuracy of the experiment. There were only 27 strains of Ralstonia pickettii and 34 strains of R. mannitolilytica out of those 152 strains selected for study by Tom Coenye et al [15]. The other 91 (59.9%) strains had relatively low species correlation with Ralstonia which were more easily and correctly to be identified. This study also showed that the 6 strains of non-Ralstonia were all identified correctly. Therefore, the PCR assays may be a reliable and simple method to identify Ralstonia pickettii, R. mannitolilytica and R. insidiosa.
Currently, there are fewer studies about the genotyping of Ralstonia [21]. Therefore, a standard MLST typing program of Ralstonia remains unestablished. Our study designed primers and determined the nucleotide sequence and performed an analysis of genotyping. The results showed that 42 strains of Ralstonia contained 18 STs and the most frequent ST was ST9 with 22 strains which are considered as the advantage type and the epidemic strain in our hospital. ST9 strains caused infections each year from 2008 to 2013. UPGMA results indicated that 42 strains of Ralstonia were grouped into 2 groups (A and B). Literature has reported identification difficulties of R. insidiosa and Ralstonia pickettii due to the close similarity [10]. As the cluster analysis shows, the R. insidiosa was in ST18, group B had a close genetic relationship with Ralstonia pickettii. But in this study, its ST code was 1-1-2-1-1-1 which was obviously different from those of the other strains in this study and consequently can be easily distinguished. However, the ST code of strain HXK003 and HXK042 were both 2-2-2-2-2, the identification result showed that they’re R. mannitolilytica and Ralstonia pickettii respectively. Our study failed to distinguish them. Due to the inconsistency between the identification result by 16 S rDNA and MLST results, it is considered to construct a two-stage MLST typing system based on 16 S rDNA. What’s more, because the strains of single source are always similar, additional gene locus are needed in the request for higher resolution, which should be further evaluated and screened.
Systematic antibiotic susceptibility data for Ralstonia Spp are scarce. Nevertheless, several studies and case reports suggested that most Ralstonia Spp are susceptible to commonly used antibiotics [22,23,24], but the result of the antibiotic susceptibility test using E-tests and broth microdilution method on 53 strains of Ralstonia pickettii by Ryan MP showed that the strains had high resistance to gentamicin and aztreonam, different degrees of resistance to ticarcillin/clavulanic acid and had sensitivity to antibiotics such as quinolones, tetracyclines, cephalosporins and sulfamido. Most of the strains were sensitive to Meropenem [22]. However, the results did not quite agree with our study. Almost all Ralstonia pickettii isolates were susceptible to cefepime, levofloxacin and Trimethoprim/Sulfamethoxazole and highly resistant to amikacin, gentamicin, aztreonam and meropenem both with the disc diffusion tests and broth microdilution method. However, poor correlation was found with piperacillin, piperacillin/tazobactam, imipenem and ciprofloxacin between MIC and disc diffusion results. Similar variation was found in the results of Ryan MP [22] and a comparable study that was carried out on Stenotrophomonas maltophilia [25, 26].
However, there was another interesting finding. As carbapenems, the susceptibilities of strains to imipenem and meropenem were strikingly different both with the disc diffusion tests and broth microdilution method. The isolates showed significantly high resistant to meropenem while much less resistant to imipenem. Especially for the disc diffusion tests, nearly half of the isolates were susceptible to imipenem, but none of the isolates were susceptible to meropenem, which might be attributed to the heavy use of meropenem in our hospital. That might indicate Ralstonia pickettii can acquire drug resistance in some way under the antibiotic pressure, which needs further studies.
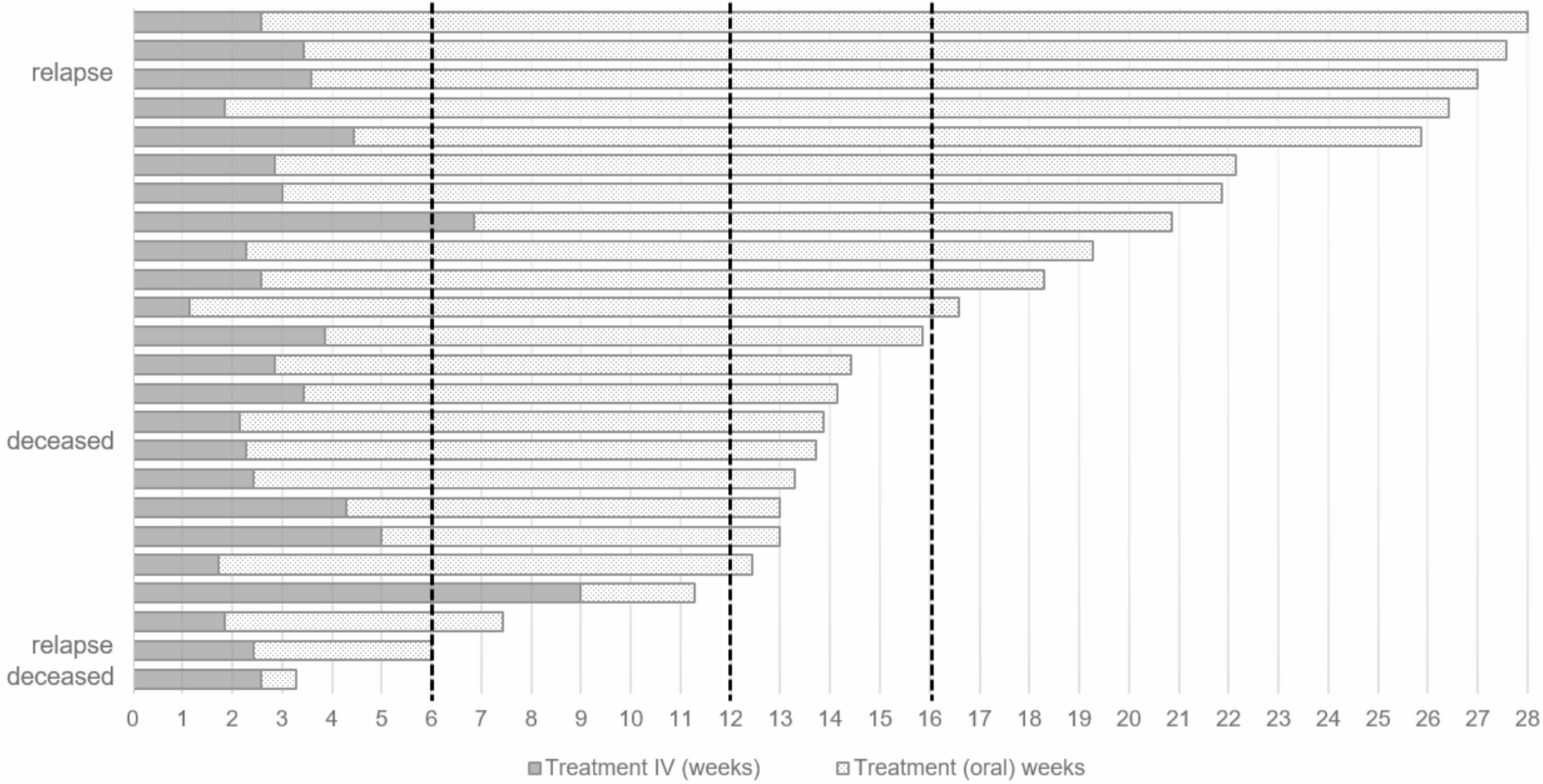
In our study, we retrospectively analyzed the clinical data of 30 elderly patients infected with Ralstonia pickettii. According to our results, the most common features of patients were cough, sputum, shortness of breath, pulmonary rales, high blood NEUT%, CRP concentration and bilateral pulmonary infiltration. These findings were consistent with hospital acquired pneumonia (HAP) in elderly patients and did not have any specific characteristics. Empirical treatment for Ralstonia pickettii infection had not yet reached any consensus. For Ralstonia pickettii strains that were less responsive to multiple antibiotics in our study, the strategy of combination antibiotics was proven to be useful, but it might also give rise to the appearance of multidrug-resistant bacteria. Ralstonia pickettii is an opportunistic pathogen especially in the hospital setting. It is a waterborne microorganism that can survive in any kind of water source and tends to form and maintain biofilms. Most of the patients in this study were elderly and had a long hospital stay. Long-term medical interventions, including the use of broad-spectrum antibiotics, deep venous catheterization, dialysis and mechanical ventilation, increased the risk of infection with Ralstonia pickettii, especially in patients infected with multi-drug resistant bacteria. These factors may lead to infections and the difficulties of removing of Ralstonia pickettii. However, our results have some limitations. The incidence and drug-resistant of Ralstonia pickettii could vary among different countries, regions, or even hospitals, giving rise to significant bias. Moreover, the clinical data was collected retrospectively so that some details on patients’ symptoms could be lost. Therefore, further researches are still needed to discover more detailed features of Ralstonia pickettii infections.
The specific PCR experiment in this study was reliable and simple, therefore, it can be used as a method to identify the clinically pathogenic bacteria of Ralstonia and provide references for clinical diagnosis. This study tried to investigate the MLST typing on Ralstonia and preliminarily establish Ralstonia ‘s MLST system to provide references for its genotyping to facilitate Ralstonia ‘s origin-tracing of its infections, especially outbreaks inside the hospital, as well as the study on its population structure. There was no specific clinical manifestations for Ralstonia pickettii pneumonia, the antibiotics should be chosen in reason according to the result of the drug susceptibility test due to Ralstonia pickettii’s resistance to various antibiotics.

Comments (0)