
Remember me







Approximately 63,000 people live with HIV in Canada (Public Health Agency of Canada, 2020). In Canada, 1 in 35 people identify as African, Caribbean, or Black (ACB) and yet one of every seven people living with HIV (PWH) identify as ACB (Mbuagbaw et al., 2022). Although the overall rates of HIV are declining, ACB women living with HIV (WWH) are significantly and disproportionately affected and at risk when compared with their non-ACB counterparts.
BackgroundAfrican, Caribbean, or Black WWH are vulnerable to experiencing the intersections of many forms of stigmatization. These forms of stigmatization are not limited to but commonly include HIV stigma (Centers for Disease Control and Prevention [CDC], 2021), racism (Ford, 2017), sexism (Iriarte et al., 2021), transphobia or homophobia (CDC, 2022), and COVID-19–related stigmatization (Hall et al., 2021; Nydegger & Hill, 2020). Intersections of stigma relates to stigmatization of varying identities and is a notable research gap within the literature (Logie et al., 2018). The layered impact of intersecting stigma and discrimination increases individual susceptibility to acquiring HIV by predisposing individuals to the impacts of the social determinants of health (Mbuagbaw et al., 2022).
HIV stigmatization often stems from a lack of education and awareness of HIV-related knowledge from both health care providers and community members who interact with people living with and/or affected by HIV (CDC, 2021). In particular, HIV stigma can have negative health consequences for ACB WWH because it can prevent women from seeking care, in addition to increasing an individual's susceptibility to depression or other mental health comorbidities (Logie et al., 2019).
Racism is the discrimination against an individual on the basis of race. Racism positively correlates with HIV stigma and has detrimental consequences for an individual's well-being (Chenneville et al., 2023; Hall et al., 2021; Mbuagbaw et al., 2022). The combined impact of HIV stigma and racism is reported by Logie et al. (2017a); however, it remains largely understudied. For example, the reported HIV stigma among WWH was found to be higher in ACB women than in white women (Logie et al., 2016). Racism affects an individual's social support network and experience of internalized HIV stigma (Chenneville et al., 2023; Logie et al., 2016). The impacts of racism are multifaceted and increase an individual's vulnerability to housing insecurity, stigma in local communities, and poverty (Chenneville et al., 2023; Hall et al., 2021; Logie et al., 2016; Nydegger & Hill, 2020). Canadian statistics show that people who identify as ACB compose 7.2% of the incarcerated population in Canada yet only 3.5% of the overall population (Canadian Civil Liberties Association [CCLA], 2021). In addition, in Vancouver, 5% of random street checks were with ACB individuals yet ACB people in Vancouver represent less than 1% of the population (CCLA, 2021). These statistics suggest that racism within Canada manifests as stigmatization and profiling of ACB populations that results in disproportionate and discriminate policing of Black Canadians (CCLA, 2021; Government of Canada, 2021). The CCLA (2021) highlights that “these trends persist even after you factor out other individual characteristics that might lead to higher levels of police contact, including living in a high-crime community, age, gender, social class, victimization, illegal drug use, criminal history, or routine activities.” (p.4)
Sexism discriminates against individuals on the basis of their sex and is commonly perpetrated toward ACB women (Taylor & Richards, 2019). Carter et al. (2014) found that quality of care services is higher among men living with HIV, and WWH are likely to face additional barriers to care. Sexism combined with the impact of HIV stigma and racism has a negative impact on overall well-being (Logie et al., 2013,2018). It is essential to understand how sexism interacts with other forms of discrimination to impact health outcomes for ACB WWH. A unique manifestation of sexism and racism was named misogynoir, referring to the ways sexism and racism commonly intersect and discriminate against ACB women (Bailey & Trudy, 2018).
In addition to sexism, transphobia is another form of discrimination. Transphobia is the stigmatization of an individual based on their self-identified status as a person whose gender identity differs from their assigned sex at birth. Transgender women are at a high risk for HIV exposure; 19.9% of transgender women in Canada live with HIV (Lee, 2022). An individual who is transgender may or may not have started the gender-affirming process through social, hormonal therapy, and/or surgical processes. Transphobia is associated with decreased adherence to HIV treatment plans and often prevents individuals from seeking HIV care services (Lacombe-Duncan et al., 2019). Transgender individuals often experience trauma within the health care system and may have depression or posttraumatic stress disorder from these experiences or from their lack of access to HIV care (Lacombe-Duncan et al., 2020). Gender-affirming health care resources can significantly improve treatment adherence to HIV care plans and mental health (Lacombe-Duncan et al., 2020; Teti et al., 2021).
Finally, by the nature of the spread of coronavirus that characterized the COVID-19 pandemic, many people experienced the effects of isolation. The isolation and resulting fear that was produced within communities had devastating consequences for isolated individuals' well-being (Nitpolprasert et al., 2021). Since COVID-19 disproportionately affected racialized and economically disadvantaged individuals, many people felt that they were avoided and further ostracized based on the way that they appeared to others (Hall et al., 2021; Nydegger & Hill, 2020). In addition, histories of endemics such as Ebola, further ostracized ACB communities during the COVID-19 pandemic; this added layer of stigmatization further increased the negative impact of all stigmatization experienced on their health outcomes. With limited evidence on the impact of COVID-19 on ACB WWH, particularly relating to their experiences of intersecting stigma, this article seeks to explore the impact of these intersecting stigmas related to the marginalized identities of ACB WWH, in addition to further understanding how this has affected their lived experience during the COVID-19 pandemic.
Theoretical FrameworkThe intersectionality framework is a dynamic, ever-evolving, socially constructive framework that builds on Black feminist thought (Collins, 1991). It posits that the experiences of women of color intersect and are affected by other identity patterns such as racism and sexism. Thus, multiple individual characteristics and identities at the microlevel (e.g., race, gender, sexual orientation, class) can act interdependently and synergistically to explain possible unifying characteristics and disparities in well-being, within such individuals and between them and others. These intersecting individual identities at the microlevel interact with larger social structures within the ecosystem to further influence human behaviors. This framework was described in the context of domestic violence experiences of women of color. According to this framework, intersectionality with ethnicity, self and/or socially assigned group identity can occur structurally, politically, and representationally (Crenshaw, 1991).
Structural intersectionality highlights the experiences women of color face when social determinants, such as poverty, education, and unemployment, intersect with their skin color to place them at a disadvantage. Political intersectionality posits that the peculiar challenges of women of color are underrepresented in ongoing political movements and their experiences are merged into those of men regardless of their (women's) unique experiences. Concerns about representational intersectionality stemmed from the underrepresentation of women of color in existing antiracism and feminism movements. Similar to domestic abuse, living with HIV is a highly stigmatized health condition. Living with HIV could further intersect with race, sex, and other variables to potentiate stigma.
We adapted this framework and applied it to this study on the intersection of stigma with racism, sexism, and other identities among ACB WWH. We also explored these stigma experiences in the context of the COVID-19 pandemic.
Methods DesignA qualitative descriptive approach (Sandalowski, 2000) was used to conduct this study to ensure rich data were collected uniquely to each participant's experience. A total of 18 participants were engaged in in-depth, one-on-one interviews lasting approximately 60–90 minutes. Data were then transcribed verbatim and analyzed using a thematic content analyses approach (Creswell & Poth, 2018).
Setting and ParticipantsWe recruited community members with lived experience of HIV, who identified as women, were living in the province of British Columbia, diagnosed with HIV at least 3 months before the start of the COVID-19 pandemic in January 2020, and were at least 16 years old. Interviews were completed between January 2022 and October 2022.
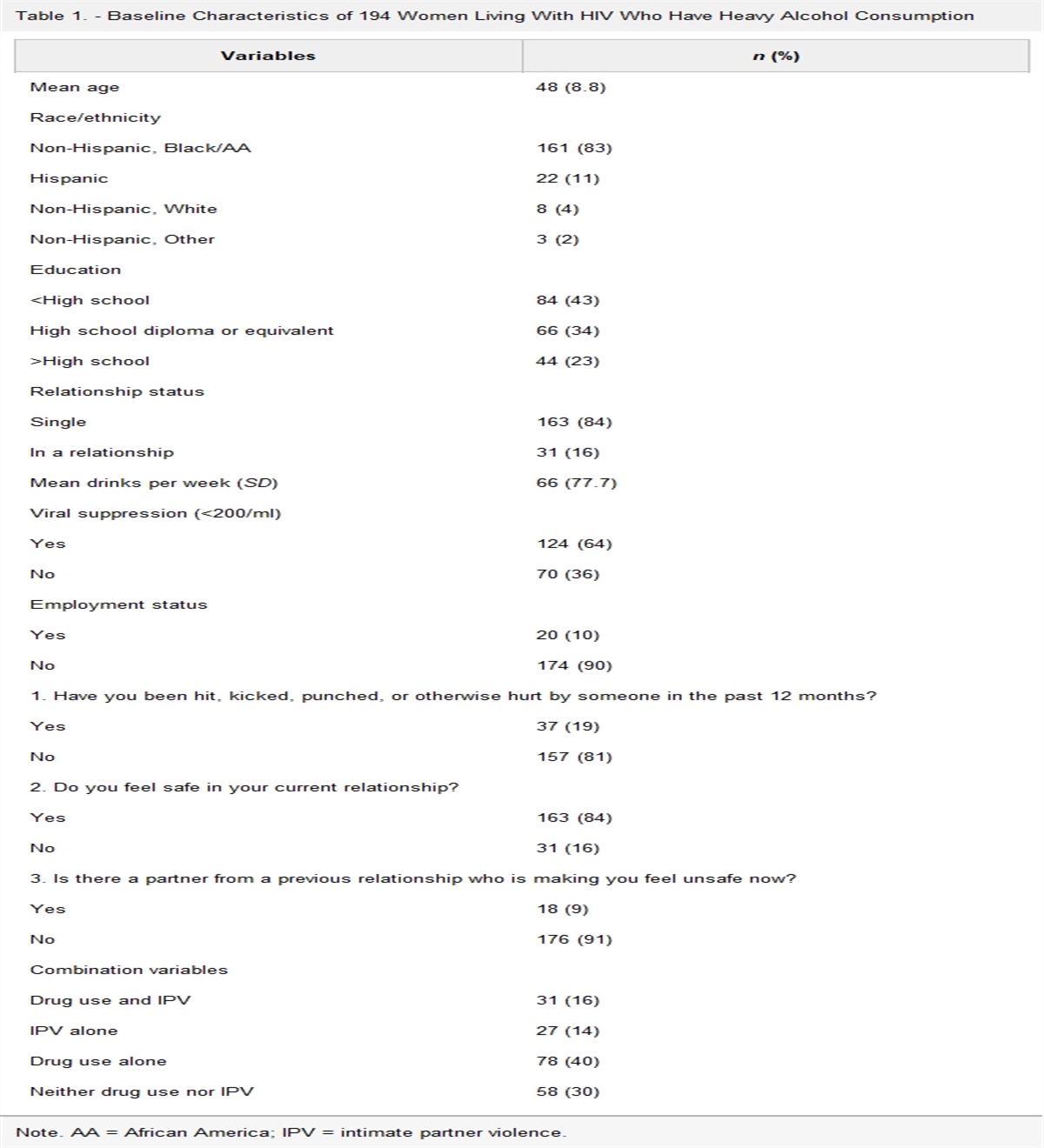
Participants chose to complete the interview over Zoom, phone, or in-person at a mutually convenient and private location. An honorarium of $40 was given to participants at the conclusion of the interview. Before beginning each interview, the researcher ensured that voluntary, informed consent had been obtained and the participants were provided a private, nonjudgmental, safe space where they could speak freely. For Zoom and phone interviews, participants were always asked about the nature of their environment and if they could speak freely therein, before the interview started. The research team also ensured bracketing (Creswell & Poth, 2018) throughout the process of the interview. Demographic information, displayed in Table 1, was collected from participants who qualified for the study and provided informed consent. One participant was not interviewed due to their ambiguity and/or unwillingness in confirming a BC residence. Interviews were audiorecorded and transcribed using Otter AI software and then manually examined for transcription errors by members of the research team. Researchers listened to the audio recording as they cross-checked the AI-generated transcript for accuracy. All noted errors were duly corrected.
Table 1. - Demographic Information of Study Participants Variable n (%) Age M = 46.9; range = 21–71 Income M = 1,861.8; range = 600–4,000$ No. of years living with HIV M=14.1; range = 4–26 Gender Cisgender 17 (94) Transgender 1 (6) Sexual orientation Heterosexual 18 (100) Racial identity African 10 (55) Caribbean 1 (6) Black 1 (6) African/Black 6 (33) Work status Full-time 8 (22) Part-time/casual 4 (45) Unemployed 6 (33) Resident status in Canada Citizen 6 (33) Permanent resident 11 (61) Student 1 (6)We used both purposive and snowball sampling techniques. Purposive sampling was achieved through posters and flyers that were distributed both electronically and manually to women's clinics, ACB communities, and HIV clinics in the province.
Community partnerships were also formed with relevant HIV support groups and organizations for ACB WWH in the province, for example, the Afro-Canadian Positive Network of BC. Within these community organizations/groups and clinics, further samples were recruited through snowballing techniques.
Data CollectionA detailed screening approach was used to determine the eligibility of participants who expressed interest in the study and their alignment with the stated inclusion criteria. To make sure the chosen participants represented the target demographic of ACB WWH during the COVID-19 pandemic in British Columbia, the principal investigator (E.O.) or the research assistant (E.M.) conducted this screening. Informed consent was obtained from each participant before beginning the interview and before the collection of demographic information. This critical ethical stage included a thorough discussion of the study's goals, methods, potential dangers, and advantages, as well as the participants' rights to confidentiality and informed consent. This made sure that everyone who agreed to participate in the study was informed and gave their consent voluntarily. Both the main investigator (E.O.) and the research assistant (E.M.) performed the in-depth interviews using a semistructured interview guide. This manual was carefully created to enable a thorough examination of the experiences of the participants. It covered a variety of topics, including dealing with HIV during the COVID-19 pandemic, the effects it had on their quality of life, and the complex interactions between overlapping identities such as race, sex, gender, HIV stigma, and COVID-19 stigma. The interviews' semistructured format allowed for flexibility while assuring uniformity between interviews. It allowed participants to express their viewpoints and personal stories while directing the conversation toward the main subjects of the study. Before being used to gather data, the interview guide was pretested to improve its clarity and suitability. The purpose of the data collection procedure was not only to document the overt experiences but also to delve into the subtleties of how intersecting discrimination and stigma affected the participants' access to HIV care and their general well-being during the pandemic. A thorough examination of the research objectives was made possible by the interviewers' use of a semistructured approach, which enabled the collection of rich and contextualized material. The study aimed to increase the reliability of its findings by ensuring transparency, ethical considerations, and rigor in the collection of data from ACB WWH participants in the context of the COVID-19 pandemic in British Columbia.
Data AnalysisThe precise transcription of the interviews, which was diligently performed by both E.M. and E.O. using Otter AI software, served as the starting point for the data analysis procedure. The subsequent analysis used a thematic content analysis approach (Creswell & Poth, 2018). Thematic content analysis was selected because it was effective at identifying and categorizing the patterns and themes present in the qualitative data. Independently, E.O. and E.M. worked through an iterative open coding process where each data segment was carefully inspected and given a tentative code. These codes were then put into more general categories and themes, allowing recurrent patterns that reflected the experiences of the participants to emerge. Regular discussion between E.O. and E.M. were undertaken to increase the analysis's reliability and trustworthiness. These talks provided a forum to discuss any inconsistencies in the coding and interpretations, which encouraged a more thorough investigation of the data and produced a more precise thematic framework. The input from these sessions was crucial in coordinating interpretations and reducing stigma. A crucial step in guaranteeing the credibility of qualitative research—member verification—was crucial to the validation of the findings. Participants received their transcribed data and the preliminary findings of the thematic analysis at this phase. Participants had the chance to evaluate the relevance and congruence of the identified themes with their own personal experiences through open discussion. Participants declared that the analysis accurately captured the essence of their experiences during the COVID-19 epidemic and confirmed the validity of the retrieved themes through this member verification process. Their support increased the validity of the study's conclusions and ensured that the data and its interpretation were in agreement. Participants shared their perspectives on the COVID-19 pandemic's effects on their life and its implications for pandemics affecting ACB WWH in the future. The research method served as the inspiration for this reflection, which not only confirmed the results but also enhanced the research by including the participants' opinions in the suggestions for potential solutions. The process of data analysis used in this study was, in essence, thorough and rigorous, including transcription, thematic content analysis, discussions among researchers, and participant validation. This multimodal strategy made sure that the results appropriately reflected ACB WWH experiences during the COVID-19 epidemic and upheld the validity of the study's findings.
Ethics ConsiderationsEthics approval was obtained from the University of British Columbia Behavioral Research and Ethics Board (H21-03210). Relevant data were kept private and confidential. All data were stored in secured university-affiliated, encrypted, password-protected, cloud storage, and password-protected computers. Paper consent forms were locked in cabinets in the affiliated university office of the study PI. Only team members who had completed the ethics training and were involved in data collection and analyses had access to the data.
Results Sample CharacteristicsA total of 18 participants self-identifying as ACB WWH were recruited in the study. Ninety-five percent identified as cisgender, and all identified as heterosexual. One participant commented on their experiences of homophobia, which intersected with their transitioning gender identity. All participants had been living with HIV between 4 and 26 years and within the ages of 21–71 years. Table 1 shows the sample characteristics.
The results of the study have been grouped into the various forms of stigma and discrimination, with exemplar quotes directly from participants and how they perpetuated suboptimal quality of life for ACB WWH in British Columbia, Canada, during the pandemic. Participant real names have been replaced with pseudonyms.
HIV StigmaAfrican, Caribbean, or Black WWH experience stigmatization on the basis of their HIV status and lived experience. This stigmatization greatly affects their quality of life and their willingness to disclose their HIV status to their social circles (Logie et al., 2013,2017b; Stutterheim et al., 2011). Many participants discussed the fear of disclosure to their close friends and family: “Something that you [are] always afraid of is stigma. Like, even if you want to go out there and socialize with people, then something reminds you you're not like them. So you kind of hold back. And, yeah, it's not that easy’’-Quinn. In discussing the fear of disclosure, participants explained that they choose not to engage in romantic relationships due to the fear of a negative reaction or fear of having to disclose their status to the relevant other. There were also issues regarding condom use within such intimate relationships, with participants disclosing a need to protect themselves and others in intimate relationships, which was difficult because it could be met by resistance from the other parties who had difficulties accepting condom use: “I'm afraid of my situation. For me to be exposing myself to people I know about myself, I don't know about the next person that I'm going to meet. And there's some people when you meet with them, they can't accept to use this condom.”–Becky
Another participant expressed that long-term relationships were especially difficult due to their partner's perception of the reason behind their request for consistent condom use and getting checked: “If we're going to be like, sexually involved. Like you know … if you're with somebody for so long, and the one thing they will say is like, go and check ourselves. Let's say like, if you really get that really good guy, let's check ourselves before we use this … then he's going to run away and say ‘Oh, that woman so and so, that one don't go close to her.’”–Alicia
The stigmatization experienced by ACB WWH is not limited to the individual's social circle; others recalled experiences of discrimination in health care settings, especially from providers who engaged them in unnecessary probing to disclose their status, even when it was irrelevant to the care they sought: “She [vaccination nurse] was asking me in a way that I should disclose my status. The questions were leading to disclosure, that I have to disclose my status.”–Lucy
Such uncomfortable probing was also recounted by participants who shared their experiences of living with roommates and its contributing factor to their experiences of HIV stigma: “Yeah, because when I move and I go outside, and then they [roommates] will be searching in my room, they see my status to know who I am.”–Francis
“When I used to live with her, I used to hide, like, I used to set my alarm at 9 pm. And one day, she was like, why do you always set your alarm at 9 pm? So I even had to not set the alarm because I didn't want her to be like ‘I wonder what [she] is doing,’ I didn't want her to have that questioning mind. And that used to stress me a lot like, you have to hide for you to take your meds, you have to hide the meds. At times, you're always afraid.”–Quinn
In addition, participants related their experiences of HIV-related stigma to a lack of knowledge from their perpetrators: “I don't know if it's because of the race, like [country name redacted] communities [are] horrible when it comes to discrimination. Like, it's like they've been brainwashed to what they're used to. With the whole debating, like with the old HIV, they don't open their mind educational-wise to know, to know that. People taking, you know, treatment have a lower risk, right.”–Sophie
RacismThe COVID-19 pandemic coincided with increased acts of racism in addition to greater awareness of anti-Black racism specifically following the murder of George Floyd (Fine, 2021). ACB communities were acutely affected. In discussion about experiences of racism, some participants expressed grief: “I feel sad and I said we run from Africa we need to be safe, but that guy [referencing George Floyd] left his kids, his wife, everything. Was having a plan in the future, he left, he was going to help, now he's just killed, now he is in a grave.”–Maya. For some, witnessing such a tragedy brought significant fear: “Yeah, it brought so much fear … the insecurity kicks in, and you're set now questioning, how am I safe here? Like, it kind of switches your mind and you start thinking, overthinking and questioning things. Yeah, it brought in that fear.”–Quinn
“I always say this when it comes to like, like racism, I always wonder whether it's, if it's me, or with somebody else, I get a mindset of being like, ignorant, you know, like, you know, like, you get upset about it, because you're like, it's still going on. It never stops when it comes to racism. With George Floyd. I look at it and say, if it was like another race, maybe that wouldn't have happened. And I realized when it comes to us with police and black people it's scary, because they don't know what the situation could be like”–Sophie
However, others expressed mixed emotions: “ah it didn't really like surprise me with such things. For a minute, I just lost faith in the system and its painful time and experience.”–Rose
Many participants shared stories of experiencing the impact of racism in their daily lives: “Yes, I am treated differently because I live in a city …. They call you names, “go back to your country” and I think some of these … things they say, they say because you are black–.”–Ellie
There were also stories shared of perceived racial discrimination in public spaces: “My daughter and I went to shop in Walmart … and we want to buy a towel …. And right away because we stand up there, they send a security [to] just come around us … they thought maybe we want to steal something. And now they send someone just going around us. It happens a lot. When you stand up and look for something, whatever. Right away, you can see the security.”–Angela
Some participants expressed how over time, they had innervated their sensations of these negative experiences to keep it from bothering them: “I face racism a lot. And at times it triggered me, especially when I'm doing my work [referring to a job]. But it is not affecting me as much as it used to because right now I've equipped myself in a way that it doesn't, it doesn't bother me.”–Lucy
Within the context of health care delivery, one participant felt that the health care providers dismissed her pain for no apparent reason: “And also in the hospital, I asked them what can I use to numb the pain for the C-section or under the area? But they didn't give me anything. I think they told they told me yeah, they're going to give me something to numb the pain …. Like they didn't give me anything. They just told me that just for me to get comfort. But then they didn't give me anything for the pain to numb.”–Sophie.
Notably, discrimination was also experienced within racialized communities based on cultural factors and the nuanced differences in the heterogeneity of culture within the same race: “Because we don't talk about how we feel, we don't talk about our private life, then talking about HIV, it is not within our culture.”–Lucy. There were also reports of similar discrimination surrounding involvement with community work related to HIV activism and advocacy: “I'm treated differently, especially when I'm doing my work within my community because knowing our culture, our African culture, we don't talk about how I am discriminated by my own people”–Lucy. This form of racial discrimination is particularly painful for participants: “even though you're my own race they discriminate… it hurts more because it hurts me to see my own race discriminate [me].”–Jessica
Children have also been affected by the experience of witnessing such overt and public acts of racism, when asked about how racism affected her children, Angela said: “Yeah, it's really difficult the way she saw things happen to black people, it's not good. And the people have to change.” Another participant said that the fear their children expressed was very consequential: “Yeah, it really impacted almost everybody even our kids, our youth. Especially our youth, my son was so afraid he was so fearful”–Lucy.
SexismIn addition to HIV stigma and racism, ACB WWH also experience sexism or stigmatization on the basis of being a woman. Many participants indicated that sexism resulted in a disproportionate amount of shared workload and a lack of support within the work places: Yeah, because I'm a woman some people take advantage of me because I don't have the strength to fight …. What I can say is like, I'm alone. I have nobody to stand behind me.”–Francis. Another participant noted: “But you find that because a woman, they do you like, you are doing most of the work. And they just sit back.”–Ellie.
Rose noted the intersection of sexism and racism: “most of the time you are treated differently by other women of a different color.” Within society, sexism is amplified as discussed by one participant: “You know, culture has put women down. This society has come to put women down”–Jessica. Other ACB WWH also reported harassment: “But the truth is that women were always targeted all the time when it comes to that. As a woman living with HIV, people call me names, they assume… assumptions are huge, everywhere you go. So they don't know the truth about what is going on.”–Lucy. Although fewer participants reported overt experiences of sexism in comparison to racism, most of the reported experiences of sexism overlapped with another form of stigmatization.
TransphobiaMaya, a transgender ACB WWH, reported on her experiences as a part of the LGBT2Q+ community. Maya reported frequent experiences wherein they felt disrespected or discriminated against by the community while going about their day-to-day activity, including in work or religious places: “So I've been struggling here in Canada … sometimes I want to wear like a woman when you outside but this street there is many black guy here, black guys from [country name redacted]. When you wear like a woman they laugh at you, you know?” Maya also shared experiences of discrimination at work: “someone said the homo. What's the meaning of homo? I was at work moping, I hear someone say is homo.” In explaining her story, Maya also expressed deep grief: “everything is worse for me. I'm not working [anymore]. My life has changed, I don't have anyone anymore. When I was coming here, I was working. Even if I've got nothing there, I can't connect this …. Then they say you are gay … I used to go on tiktok … but even that, [my] people in [country redacted], they say to me, you are gay, you dance like a woman. Like that, they can't change me. I miss my family a lot.”
This grief intensified feelings of isolation: “Where I come from we are Muslim. Me I was like somebody who used to pray with people in that temple. So the family when they did know that I'm a gay, if everybody they lose trust in me. They lose trust to me, because I was a leader at temple then they lose trust on me. So I'm in cursed. They cursed me. Everybody, they cursed my kids, they cursed me.”–Maya.
The grief and isolation Maya experienced because of her gender and sexuality intersect with other forms of stigmatization experienced by cisgender and heterosexual ACB WWH.
COVID-19 StigmaTo reduce the spread of the COVID-19 virus, social distancing and masks were required in many parts of Canada. Although these measures were effective in limiting the spread of the virus, they also isolated people from one another and greatly limited human interaction. Measures like social distancing were not accessible for people living in shared housing or working in health care. ACB people are disproportionately affected by these constraints, in addition to the long-standing impacts of structural racism and subsequently experienced more COVID-19 infections (Hall et al., 2021; Nydegger & Hill, 2020). Some participants expressed that they felt visually targeted because of their race and others' misconceptions: “that time [COVID] was very hard … to deal with the HIV … they started [to] say these come in, they come in from African countries. That HIV [and COVID] was coming from African countries. Again that sickness [referring to monkey pox] was coming from Europe to here, you know because we are black, everything they said is coming from black people.”–Tatum
Others expressed frustrations regarding the misinformation about the COVID-19 pandemic and the fear that the misconceptions created: “So there are stereotypes about COVID and HIV … someone talking that oh people with an immune system which is compromised, they're going to die. And all those things, we're hearing so many stories in the community, but … we're struggling [with] mental health at that time” - Lucy. Sophie continued on to discuss the difficulties experienced by managing both pandemics (HIV and COVID) for people like her who also contracted COVID-19, “having to deal with this new COVID-19 while having HIV, just like two viruses … it has a stress on health, because you're trying to, like, maintain your health, following protocols and trying to prevent yourself from not getting COVID-19.”
Furthermore, the lack of information on how to effectively manage both was especially difficult to deal with and left some participants feeling powerless: “It's [COVID-19] been so traumatic, because you don't know what is true about the virus and the vaccines. You don't know what's true”–Ellie.
Intersectional StigmasThe impacts of stigmatization on the basis of race, sex, gender identity, HIV status, and the COVID-19 pandemic are complex. This article aims to reveal the unique challenges faced by ACB WWH when their identity and experience intersects with many forms of stigmatization. As described by Crenshaw (1991), the intersection between race and sex can explain the similarities in disparities and discrimination experienced by ACB WWH. These intersections can also occur between the identity as an ACB woman and HIV status, COVID-19 status, and gender identity. One participant described the way her experience of racism was intensified because of her identity as an ACB woman. In her lengthy quote below, we highlight, in italicized text within parenthesis, the different layers and intersections of stigmatization as discussed by her: “the racism [racism] has become, it became worse during COVID [COVID-impact], worse. During COVID I used to just hear racism, I'm like hmmm …. But now even your own sister when they see you sneeze [COVID-stigma], nobody's going to get close to you. They will run away … But even when you go to the store, when they see a black person, it's like you're the owner of COVID you have [it], you're the supplier, [racism and COVID-stigma]. It became so [much] worse, I used to just hear, oh, this discrimination. I never felt it. Like I felt it. I know how it feels. But it was really worse. Like when you get to deal with it, like all the time you deal with it … everywhere you go you get that feeling, it grew worse.”–Jessica
Sophie also commented on the important distinction in the way that HIV stigmatization and racism interact to create an intersection of stigma: “sometimes you can experience like discrimination based on race, because people be treated differently because of color. And different from a person who is like, not black and have HIV from a person who is black and have HIV.”
Other participants described the impact of intersecting stigmatization as the most impactful on their quality of life during the COVID-19 pandemic: “I don't know how to describe what it was, it was because I'm black living with HIV and then COVID-19 too. [It] was something unbelievable. I going to just say we thank God because of this COVID is going away now, it was terrible.”–Joy
The way different forms of stigmatization intersect for ACB WWH poses unique challenges, including isolation, grief, fear, misconceptions, profiling, discrimination in health care settings, and decreased quality of life.
Need for ResourcesThere is a unique need for resources dedicated to helping ACB WWH deal with and prevent the consequences of intersecting stigma. When asked about the availability of resources to help participants cope with racism the same way resources were available to cope with COVID-19, more than half of the participants (N = 10) said that there were no resources available or that they wished there were resources available. Claire indicated that support groups would be instrumental in facilitating community networks and connections: “I would like to have a place or supportive social place where I would go and meet people who are like me or similar to me, or, you know, like people that I can relate with in terms of my race and my culture and everything like that.” Maya also said that LGBTQ support groups for new Canadians would be very impactful. Many participants revealed that their support groups and other resources were quickly depleted at the start of the pandemic. Many other participants cited resources to address food insecurity and financial constraints as a key priority. Advocacy to end HIV stigmatization and increase government awareness of the ways that HIV impacts ACB WWH would greatly improve the quality of life. In addition, advocacy for asylum candidates and increased provision of information and resources about HIV for new Canadians would improve the experience of navigating a new HIV diagnosis. When asked about resources that could assist individuals in dealing with the impact of living with many intersecting stigmas, Francis reported that interventions focused on empowerment would be particularly helpful.
DiscussionAs described by Crenshaw (1991), the results of this article intimately describe the ways various types of stigmatization intersect for ACB WWH. The cumulative influence of HIV stigmatization, racism, sexism, transphobia and homophobia, and COVID-19 stigmatization create unique health, social, and financial disparities for ACB WWH (Figure 1). These disparities have consequences for both physical and mental health, financial security, and even more compounded experiences of isolation.
 Figure 1.:
Figure 1.: A visual representation of the intersecting stigmas experienced by ACB WWH during the COVID-19 pandemic. ACB WWH = African, Caribbean and Black women living with HIV.
In particular, experiences of racism were associated with experiences of HIV stigmatization and depression (Logie et al., 2017a). These results are consistent with the results of our study; many participants who described experiences of intersecting racism and HIV stigmatization also described mental health symptoms mirroring those of depression or anxiety. It is relevant to consider the health care context in which both studies were completed. Although the study by Logie et al., 2017a was completed in Ontario and this study in British Columbia, they are representative of different health care systems within Canada. Iriarte et al. (2021) identified factors that correlated between mental illness and ACB and Hispanic WWH who are 50 years of age or older. The primary identified mechanism to minimize mental health consequences for this population was to develop coping abilities (Iriarte et al., 2021). Our study found that social support groups were helpful in improving the experience of intersecting stigmatization. Chenneville et al. (2023) described the experience of intersecting stigmatization for youth with HIV in the Deep South of the United States. Consistent with the results of our study and other literature, Chenneville et al. (2023) identified the need for increased interventions and resources. In addition, Chenneville et al. (2023) also pointed to the experiences of racism as a cause of health disparities for ACB youth living with HIV. Ford (2017) described the ways that intersecting stigma continues to disadvantage ACB people, particularly on the basis of race and the health disparities that exist for ACB PWH in the United States. Ford (2017) also reminded the reader that disparities that exist on the basis of race are not due to an unknown causal factor, they are typically in response to different forms of discrimination experienced by an individual. Implementing psychoeducational workshops with the aim of enhancing coping strategies among ACB WWH can help them use stress reduction techniques, emotion regulation skills, and mindfulness practices.
Intersecting gender and sexuality discrimination was found in this study. Similar findings were reported in a qualitative study wherein stigma and gender discrimination were reported by transgender WWH, which increased their risk of adverse outcomes of COVID-19 due to reluctance to seek COVID-19 testing and treatment (Pandya & Redcay, 2022). A study conducted among transgender women noted health care providers' discomfort serving transgender WWH and also their vulnerability to COVID-19 harms, including losing job, reduced income, food insecurity, housing problems, and violence (Poteat et al., 2020). The idea of intersectionality illuminates how power functions at the confluence of various identities, including racial, gender, and HIV status. The combination of stigmatized identities that ACB WWH experience leads to particularly severe forms of stigma and discrimination. Their interactions with health care providers and their capacity to obtain equitable health care services are affected by complicated power dynamics created by these intersecting identities.
Intersecting gender and race discrimination were experienced by WWH because of their being both women and Black in this study. Similar findings were found in a study conducted among Black WWH in which they are discriminated against and insulted because of their identities such as jokes about their hair, body shape, voice level, and also being accused of being angry, being assertive, and getting negative comments for their natural shape of hair (Lewis & Neville, 2015). Supportive peer networks for ACB WWH can provide a space to hear peer mentors' experiences in similar challenges, exchange coping strategies, and receive emotional support.
As previously investigated by Logie et al., 2017b, we found that the impact of intersecting stigmatization posed health risks and challenges for ACB WWH and that more resources are needed to minimize the consequences to ACB WWH. Two other studies conducted among 104 WWH in Ontario, Canada (Logie et al., 2011), and 173 ACB WWH in Ontario, Canada (Logie et al., 2017b), reported similar findings in experiencing particular barriers to accessing and engaging in HIV-related care services and other health services because of intersecting stigmatization of sexism, racism, and HIV-related stigma. Symbolic interactionism, developed by Goffman (Scheff, 2005), can provide insight for the microlevel interactions and social processes that lead to experiences of ACB WWH. These views may be experienced by ACB WWH navigating health care services during the pandemic through the lens of their intersecting identities and HIV status. Health care professionals could contribute to stigma and discrimination unintentionally by nonverbal cues, word choices, and body language. The covert mechanism by which stigma is spread and reinforced affects how ACB WWH view themselves and their willingness to seek out HIV care and support services. One example is the way patients may be questioned about their status within the health care setting. In Canada, a patient's health number can provide details of their medical history from birth, whenever that number is presented at a hospital or health system. A review of a person's record through this number can often reveal their HIV status. Thus, additional patient probing for verbal validation and/or affirmation of their statuses in these situations, especially when the provider already has this information, is unnecessary and may seem judgmental, uncomfortable, and stigmatizing for the patient. Understandably, questions regarding treatment adherence and engagement are warranted to the extent that they may affect the patient's current health condition for which they have sought care. However, in the setting of a vaccination, such probing may be unwarranted because information is mostly sought regarding any known allergies to the vaccination. In our study, participant, Lucy, recounts her discomfort with such a situation during a scheduled vaccination visit. Other interventions to make health services accessible, nondiscriminatory, and accommodating of the needs of ACB WWH, such as flexibility in appointment scheduling, telehealth, and transportation assistance, can help to reduce barriers to accessing care.
An intersectional perspective acknowledges that because of the confluence of many identities and social settings, the experiences of ACB WWH cannot be understood in isolation. The discrimination and stigma they experience are amplified by the combination of race, gender, and HIV status, creating particular problems that necessitate specialized solutions. Such a strategy acknowledges that single-issue solutions cannot adequately address the experiences of ACB WWH. Instead, interventions must be planned to address stigma, discrimination, and other barriers to care holistically while taking into account the whole range of their identities and experiences.
Access to care and measures to prevent the spread of HIV are also cited as influential in informing misconceptions surrounding the increased prevalence of HIV in ACB populations. Barriers to care and minimizing the spread of HIV need to be addressed and further investigated (Ford, 2017). Additional research is needed on how public health care systems can be adapted to minimize the impact of structural racism and other forms of discrimination (Ford, 2017).
Hall et al. (2021) and Nydegger and Hill (2020) described the ways that the COVID-19 pandemic exacerbated health disparities among PWH. Consistent with the participants in our study, participants reported that the stigmatization experienced because of COVID-19 status mirrored that of the stigmatization experienced related to HIV status (Hall et al., 2021). Both Hall et al. (2021) and Shiau et al. (2020) reported increased fear of contracting the COVID-19 virus among PWH. ACB WWH in this study and similarly reported fear of the unknown impact of the COVID-19 virus and the difficulty of navigating rapidly changing public health guidance. A report by the Global Network of PWH reported stigma and discrimination from health care providers because they assume that PWH are at greater risk of contracting and spreading COVID-19, which also could affect health and well-being of PWH (Global Network of People Living with HIV, 2020). Reports of the Joint United Nations Programme on HIV/AIDS presented evidence of increase in experiencing stigma and discrimination, violence, and abuse among WWH due to COVID-19 restrictions and lockdown (Joint United Nations Programme on HIV/AIDS, 2021). Also, findings of a systematic review showed that PWH encountered several issues related to COVID-19, including intersectional stigma and discrimination, which led to the emergence of problems related to receiving medicines and adherence to treatment (SeyedAlinaghi et al., 2023).
Medical mistrust was reported by individuals in this study, which is defined as the lack of trust of WWH in health service providers following the occurrence of discriminatory behaviors. HIV status disclosure without consent and by demand of health care provider and health care provider neglecting patient's pain were reported by participants, which contribute to medical mistrust. Medical mistrust could lead to individuals' unwillingness to pursue treatment for health problems and HIV (Rintamaki et al., 2006).
In general, participants described experiencing stigma and discrimination as a result of having one or more stigmatized identity. However, they also reported that being part of a support group has helped them cope with the stigma they received. This finding is in agreement with a number of studies that have found that social support was linked to lower levels of HIV-related stigma (Emlet, 2006; Heckman et al., 2004; Logie et al., 2011; Silver et al., 2003).
Nurses are a key part of the HIV care team and can advocate for patients with HIV. Nurses need to be aware of the way that the social determinants of health and various forms of stigmatization and discrimination uniquely impact ACB WWH. Nurses can also help to guide patients through the health care system, particularly newcomers to Canada or those with language barriers. Nurses should be aware of the community resources available in their area so that they can provide patients with information about how to access support services outside of the biomedical health care model.
Nurses are particularly well positioned to address the intersectional difficulties encountered by ACB WWH and play a crucial role in the health care system. Their all-encompassing method of treatment, which emphasizes both mental and physical health, is in line with the sophisticated requirements of this demographic. Through ongoing patient interactions and the development of trusting relationships, nurses can provide safe spaces for ACB WWH to express their experiences with stigma and discrimination. By embracing the intersectionality of identities and comprehending the effects of stigma on health outcomes, nurses can promote culturally competent care. This entails attending to the medical requirements of ACB WWH in addition to acknowledging and supporting their lived experiences. Nurses can help to lessen stigma and provide an inclusive health care environment by being aware of verbal language, body language, and nonverbal signs.
Future research is needed to explore how experiences of intersecting stigmatization impact the lives of ACB WWH and how resources can be improved to address these impacts. Specifically, research into how to improve care and access to resources for ACB WWH in future pandemics is essential. Research is also needed to identify the resources needed to equip ACB WWH with the necess
Comments (0)