KEY POINTS
1) It is relevant to know how viral infections emerged after the COVID-19 pandemic, all motivated by home confinement and transmission restrictions.
2) The return to school of children and adolescents and the lifting of restrictions, conditioned the reappearance of common viral infections, although they emerged in unusual periods of the year.
3) The respiratory syncytial virus (RSV) and influenza epidemics significantly changed their seasonality. In the case of RSV, it also debuted in the fall of 2022 with a high virulence and hospitalization rate.
In response to the COVID-19 pandemic, preventative measures in the population were established globally to reduce its impact on the number of infected. These measures consisted of the use of masks, hand washing and use of antiseptics, quarantine prescription, social distance, etc.1 These measures were applied to the adult as well as pediatric population.2,3 In Spain, the reincorporation of schoolchildren and adolescents into schools and colleges, with social distancing measures and the use of masks, occurred in September 2020. The lifting of these restrictions was decided in spring 2021.
In this context, health systems noticed an apparent change in the seasonality and epidemiology of common viral infections in both the adult and pediatric populations.4 This phenomenon has been described in recent medical literature, especially throughout the period of confinement, and, to a lesser extent, in the adolescent and pediatric population after starting school.5–9 One of the epidemic changes observed in our environment was the change in the peak incidence of acute bronchiolitis.10 In a recently published review, Chow et al11 described a reduction in respiratory viral infections, including influenza virus and respiratory syncytial virus (RSV) during and after the COVID-19 pandemic. This reduction was most notable at the start of the pandemic and continued to varying degrees throughout subsequent SARS-CoV-2 infection outbreak leading to a decrease in hospitalizations and deaths associated with these viruses.11
Acute respiratory infections of viral origin constitute a significant care burden for healthcare systems, and their epidemic behavior after an unprecedented world pandemic is of substantial interest to scientific researchers. These observations could help healthcare institutions and professionals make strategic decisions regarding similar events in the future.
This observational study intends to describe the progression of the most common viral infections throughout the COVID-19 pandemic, with a focus on the changes that occurred after children and adolescents returned to school, using a retrospective analysis of polymerase chain reactions (PCRs) performed in our hospital on the pediatric population.
METHODS
We retrospectively analyzed the results of all performed respiratory virus PCRs carried out on nasopharynx samples of patients younger than 18 years attended at Clínica Universidad de Navarra (Madrid, Spain), once children and adolescents started schools and colleges in September 2020. Lockdown due to COVID-19 in Spain was decided by the government on March 14, 2020. In our region, Madrid, children, and adolescents went back to schools in September 2020 with significant restrictions to avoid contagiousness, and then these were lifted at the end of April 2021.
The viral PCR results were analyzed in 2 different periods: period 1 before COVID-19 irruption (September 2019 to February 2020) and period 2 when children came back to school and common viral infections started (September 2020 to November 2022). Period 2 results were secondarily analyzed in quarterly subperiods (Supplementary Material Table S1, https://links.lww.com/IDCP/A59). The analysis of the PCRs in period 1 aimed to obtain a comparison scenario before the outbreak of SARS-COV-2.
All nasopharynx samples had been tested with multiplex PCR assay to detect the presence of the main respiratory viruses: influenza virus, RSV, human parainfluenza viruses, human rhinovirus/enterovirus, adenovirus, human metapneumovirus, common coronaviruses, and human bocavirus. For this purpose, 2 multiplex PCR assays were used: Allplex Respiratory Panel Assays (panel 1, panel 2, panel 3) (Seegene, Seoul, South Korea) and FilmArray Respiratory Panel 2.1 (RP2.1) (BioFire Diagnostics, Salt Lake City, Utah). Rhinoviruses and respiratory enteroviruses are classified in the Enterovirus genus within the Picornaviridae family: both share similarities in their genome and were detected simultaneously. The epidemiological data associated with PCR samples as age, sex, and hospital admission (yes/no) were obtained from electronic medical records.
All statistical analyses were performed using Stata/IC version 12.0 statistical software (StataCorp, Tex). Categorical variables are reported as frequencies and percentages, and continuous variables are reported as medians and interquartile range (IQR). The statistical relationship between categorical variables was calculated through the development of cross tables and the calculation of the χ2 test. Continuous variables were analyzed with nonparametric tests (Wilcoxon rank sum test). P value was considered statistically significant when less than 0.05. The study protocol was approved by the University of Navarra Ethics Committee with the code 2023-046.
RESULTS
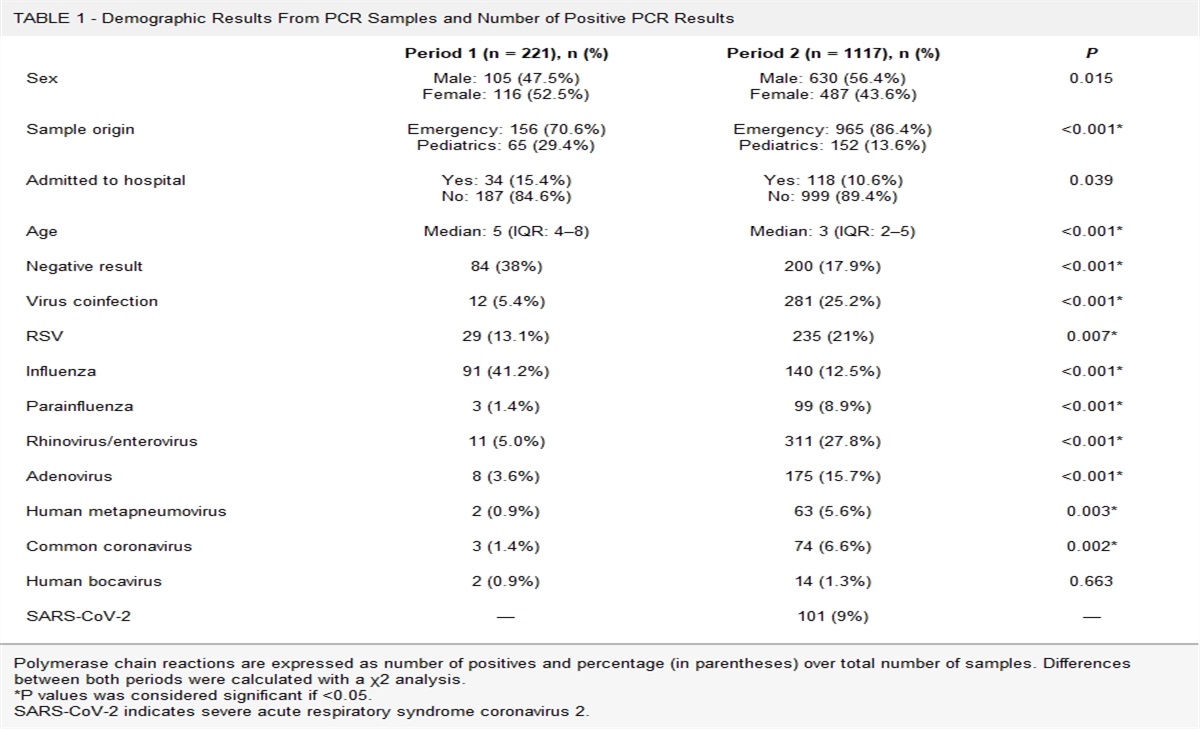
A total of 1338 respiratory virus PCR results from our microbiology laboratory were reviewed. Of the total, 221 corresponded to samples along period 1 (pre–COVID-19), and 1117 to samples obtained along period 2. Demographic aspects of all samples are summarized in Table 1. For samples from period 2, most of them were derived from the pediatric emergency department (86.4%). During period 1, before COVID-19 lockdown, there was a higher percentage of negative samples (84, 38%) than in period 2 (202, 17.9%) (P < 0.05). Conversely, there was a higher percentage of co-infections in period 2 (25.2% vs 5.4%, P < 0.05).
TABLE 1 -
Demographic Results From PCR Samples and Number of Positive PCR Results
Period 1 (n = 221), n (%)
Period 2 (n = 1117), n (%)
P
Sex
Male: 105 (47.5%)
Female: 116 (52.5%)
Male: 630 (56.4%)
Female: 487 (43.6%)
0.015
Sample origin
Emergency: 156 (70.6%)
Pediatrics: 65 (29.4%)
Emergency: 965 (86.4%)
Pediatrics: 152 (13.6%)
<0.001*
Admitted to hospital
Yes: 34 (15.4%)
No: 187 (84.6%)
Yes: 118 (10.6%)
No: 999 (89.4%)
0.039
Age
Median: 5 (IQR: 4–8)
Median: 3 (IQR: 2–5)
<0.001*
Negative result
84 (38%)
200 (17.9%)
<0.001*
Virus coinfection
12 (5.4%)
281 (25.2%)
<0.001*
RSV
29 (13.1%)
235 (21%)
0.007*
Influenza
91 (41.2%)
140 (12.5%)
<0.001*
Parainfluenza
3 (1.4%)
99 (8.9%)
<0.001*
Rhinovirus/enterovirus
11 (5.0%)
311 (27.8%)
<0.001*
Adenovirus
8 (3.6%)
175 (15.7%)
<0.001*
Human metapneumovirus
2 (0.9%)
63 (5.6%)
0.003*
Common coronavirus
3 (1.4%)
74 (6.6%)
0.002*
Human bocavirus
2 (0.9%)
14 (1.3%)
0.663
SARS-CoV-2
—
101 (9%)
—
Polymerase chain reactions are expressed as number of positives and percentage (in parentheses) over total number of samples. Differences between both periods were calculated with a χ2 analysis.
*P values was considered significant if <0.05.
SARS-CoV-2 indicates severe acute respiratory syndrome coronavirus 2.
There were differences in the percentage of positive PCR results before and after school restrictions in April 2021. A summary of these results can be consulted in Table 2. Influenza, SARS-CoV-2, and human bocavirus viruses showed an increase in the period with the lifting of restrictions at school (P < 0.05). Conversely, the lifting of restrictions decreased the number of positives PCRs for rhinovirus/enterovirus, RSV, common coronavirus, and human metapneumovirus (P < 0.05).
TABLE 2 -
Summary of Positive Viral PCR, in Relation With Lift of Restrictions at Schools
YES Restrictions at Schools, n (%)
No Restrictions at School, n (%)
P
Negative result
120 (17.1)
80 (19.2)
0.389
Virus coinfection
181 (25.9)
100 (24.0)
0.485
Adenovirus
105 (15.0)
70 (16.8)
0.389
Rhinovirus/enterovirus
247 (35.3)
64 (15.3)
<0.001*
Parainfluenza
59 (8.4)
40 (9.6)
0.508
RSV
165 (23.6)
70 (16.8)
0.007*
Common coronavirus
55 (7.9)
19 (4.6)
0.032*
Influenza
75 (10.7)
65 (15.6)
0.017*
SARS-CoV-2
51 (7.7)
50 (12.2)
0.004*
Human metapneumovirus
49 (7.0)
14 (3.4)
0.011*
Human bocavirus
0 (0)
14 (3.4)
<0.001*
Differences were calculated with a χ2 analysis
*P values was considered significant if <0.05.
During period 1, the most identified virus was influenza (91; 41.2%), followed by RSV (29, 13.1%). During period 2, the most frequently identified virus was rhinovirus/enterovirus (311, 27.8%), followed by RSV (235, 21%) and adenovirus (175, 15.7%). The rest of the identified viruses are detailed in Table 1.
The secondary analysis of positive PCRs during period 2 by quarter periods showed the following results. A summary of the number of positive PCRs, out of the total PCRs performed, distributed by quarterly periods can be consulted in table S1 (supplementary material, https://links.lww.com/IDCP/A59). In March 2021, coinciding with an increased number of pediatric patients attending the emergency department (Fig. S1, supplementary material, https://links.lww.com/IDCP/A59), our hospital began to perform a higher number of viral PCR tests.
From March to August 2021, a noticeable number of cases of RSV infection were observed. From March to May 2021, 58.9% of the positive PCRs were positive to RSV. Similarly, in the next quarter from June to July 2021, 38.1% of the positive PCRs were positive to RSV.
The percentage of positives rhinovirus/enterovirus PCRs is maintained at high levels over the total samples almost constantly in almost all quarters, especially standing out between September and November 2021. A significant peak in the summer of 2021 is also noteworthy. The influenza virus presented the peak of the highest percentage of positives out of the total PCR tests analyzed between March and May 2022 (72; 36.4%).
DISCUSSION
Our study shows a summary of positive PCR data of the most common respiratory viruses collected in our center, as a reflection of their epidemic circulation, in relation to COVID-19 pandemic. Our main results show that there were differences in the percentage of positive PCR results before and after school restrictions in April 2022. These results coincide with those provided by other authors, from the perspective of the impact of the return to school in the pediatric population in our environment that took place in September 2020.1,10 In accordance with guidelines published by the regional government, the return to school took place with a series of restrictions to prevent further transmission of infections in schools and colleges (ventilation of spaces, vaccination recommendations, hand hygiene, use of masks in people older than 6 years). Our data reflected that the number of samples collected increased from March 2021, which coincided with the increase in the number of pediatric patients who were attended in our emergency department. Initially, after children and adolescents returned to school, measures to prevent the transmission of respiratory infections were likely maximized, leading to a lower number of viral infections in a period where numerous respiratory infections are usually seen.
Our results show a change in the seasonality of RSV infections. In our environment, in southern Europe, the epidemic period usually begins in October and ends in March12 and yet the highest percentage of positives for this virus was delayed in our laboratory results until the months of spring and summer. This effect has also been described by Bermúdez Barrezueta et al10 in our setting when analyzing hospital admissions for acute bronchiolitis. They observed that the first case requiring admission for acute bronchiolitis was in April 2021. These authors also describe a peak of infection in July 2021, during the middle of summer, with a 60.7% decrease in the need for admission for this pathology. Guitart et al13 also describe this effect in the literature, noting a dramatic drop in Pediatric Intensive Care Unit admissions for bronchiolitis during the 2020–2021 season. They also observe prepandemic and postpandemic changes in the age of admission (higher in the post–COVID-19 period), length of hospitalization, or length of stay in the pediatric intensive care unit (lower in the post–COVID-19 period). This effect is also described in the southern hemisphere by Eden et al.14
We also observed a change in the seasonality of the influenza virus with late epidemic peaks between March and May 2021, and almost nonexistent changes in the winter and spring of 2020. Ye et al15 described in Asia, in a retrospective study on massive numbers of microbiological samples taken between 2019 and 2020, an epidemiological change in respiratory viruses, describing a higher rate of RSV positives in 2020 (69.1%), and a lower presence of adenovirus and parainfluenza. Liu et al4 also described an increase in RSV in hospitalized patients, including those older than 12 months, in which rhinovirus had predominated the previous year.
Both behaviors for the fall of 2022, both for the influenza virus and the RSV, were predicted by the Centers for Disease Control and Prevention.16 According to epidemiological surveillance systems, 2 influenza epidemics were observed in Spain in 2022, one during its usual period and the second later and for a longer period than in previous seasons, with a predominance of the A strain (H3N2).17 In the 2021–2022 season, there was an epidemic of RSV with a peak incidence between week 49/2021 in hospitals and week 1/2022 in primary care, which reproduces seasonal patterns from seasons prior to the COVID-19 pandemic. This peak between 2021 and 2022 is reflected in our results. However, in Spain, the behavior of RSV between the months of October and December 2022 has been markedly virulent, leading to numerous admissions to hospitals, and occupation of beds in pediatric intensive care units. Normally, the peak of the highest incidence of RSV infection occurred in the last week of the year and the first week of the following, and it came earlier in 2022.17,18 This is confirmed in the Spanish epidemiological surveillance report as of January 2023, which shows a strikingly higher rate of hospitalization due to confirmed RSV infection in week 48.19 This last peak is not reflected in our results because of our hospital's reduction of performing random respiratory panels in the emergency department from December 2022 brought on by issues from the health management department.
Undoubtedly, all these changes in seasonality and virulence of respiratory viruses in the child population in our environment have been motivated by the COVID-19 pandemic, but also by the restriction measures aimed at its prevention, in schools. For the authors, it is important to know these epidemiological behaviors to understand what will happen in the future in a similar situation, which involves the confinement of the population, the lower circulation of certain common viruses, and the use of restrictive measures for infection transmission among schoolchildren.
One main limitation of this study is determined on how results are obtained. These are based on a retrospective analysis of PCR results from samples taken randomly from our pediatric and emergency departments. Samples were taken during the febrile period of the infection attended in Accidents & Emergencies due to the awareness of parents at this stage in the pandemic. From that point of view, our random samples can be a reasonable good reflection of the epidemic behavior of common virus.
We conclude that with the end of the COVID-19 pandemic, and after the reincorporation of children and adolescents to schools, the circulation of common viruses in this age group increased gradually, with an unusual delay and epidemic peaks outside the usual periods. The authors of this study believe that knowledge of these viral seasonal changes is relevant to understand, predict, and respond in the future to a similar epidemiological context.
REFERENCES
1. Achangwa C, Park H, Ryu S, et al. Collateral impact of public health and social measures on respiratory virus activity during the COVID-19 pandemic 2020–2021. Viruses. 2022;14(5):1071.
2. Merino-Navarro D, Díaz-Periánez C. Prevention and treatment of COVID-19 in the pediatric population from the family and community perspective. Enferm Clin. 2021;31:S29–S34.
3. Garcia-Alamino JM. Epidemiological aspects, clinic and control mechanisms of SARS-CoV-2 pandemic: situation in Spain. Enferm Clin. 2021;31:S4–S11.
4. Liu P, Xu M, Cao L, et al. Impact of COVID-19 pandemic on the prevalence of respiratory viruses in children with lower respiratory tract infections in China. Virol J. 2021;18(159):1–7.
5. Chen YJ, Er TK. Distribution of viral respiratory infections during the COVID-19 pandemic using the FilmArray Respiratory Panel. Biomedicine. 2022;10(11):2734.
6. Nunes-Silva C, Vilares AT, Schweitzer V, et al. Non-COVID-19 respiratory viral infection. Breathe (Sheff). 2022;18(1):210151.
7. Montejo M, Sánchez A, Paniagua N, et al. Reduction in the incidence of acute bronchiolitis and related hospital admissions during the COVID-19 pandemic. An Pediatr (Engl Ed). 2022;96(6):537–539.
8. Gandhi L, Maisnam D, Rathore D, et al. Respiratory illness virus infections with special emphasis on COVID-19. Eur J Med Res. 2022;27(1):236.
9. Yuen E, Gudis DA, Rowan NR, et al. Viral infections of the upper airway in the setting of COVID-19: a primer for rhinologists. Am J Rhinol Allergy. 2021;35(1):122–131.
10. Bermúdez Barrezueta L, Gutiérrez Zamorano M, López-Casillas P, et al. Influence of the COVID-19 pandemic on the epidemiology of acute bronchiolitis. Enferm Infecc Microbiol Clin. 2023;41(6):348–351.
11. Chow EJ, Uyeki TM, Chu HY. The effects of the COVID-19 pandemic on community respiratory virus activity. Nat Rev Microbiol. 2023;21(3):195–210.
12. Barr F, Graham B. Respiratory syncytial virus infection: clinical features and diagnosis. In: UpToDate, Inc. 2022. Available at:
http://www.uptodate.com. Accessed March 30, 2023). doi:10.1097/00063198-200205000-00011
13. Guitart C, Bobillo-Perez S, Alejandre C, et al. Bronchiolitis, epidemiological changes during the SARS-CoV-2 pandemic. BMC Infect Dis. 2022;22(1):84. doi:10.1186/s12879-022-07041-x.
14. Eden JS, Sikazwe C, Xie R, et al. Off-season RSV epidemics in Australia after easing of COVID-19 restrictions. Nat Commun. 2022;13(1):2884.
15. Ye Q, Liu H. Impact of non-pharmaceutical interventions during the COVID-19 pandemic on common childhood respiratory viruses—an epidemiological study based on hospital data. Microbes Infect. 2022;24:104911.
16. Tanne JH. US faces triple epidemic of flu, RSV, and COVID. BMJ. 2022;379:o2681.
17. Delgado-Sanz C, Mazagatos C, Díaz R, et al. Del Instituto de Salud Carlos III. Informe anual SiVIRA de Vigilancia de gripe, COVID-19 y VRS. Temporada 2021-22. Disponible en: Gripe, COVID-19 y otros virus respiratorios (isciii.es). 2022.
18. Jiménez-Jorge S, Delgado-Sanz C, de Mateo S, Pozo F, Casas I, Larrauri A. Monitoring respiratory syncytial virus through the Spanish influenza surveillance system, 2006–2014. Enfermedades Infecciosas y Microbiología Clínica. 2015;34(2):117–120.
19. Instituto de Salud Carlos III. Vigilancia centinela de Infección Respiratoria Aguda en Atención Primaria (IRAs) y en Hospitales (IRAG) en España. Gripe, COVID-19 y otros virus respiratorios. Semana 01/2023. No. 113. 11 de enero de 2023.







Comments (0)