
Remember me

This target trial emulation used data from three prospective longitudinal multicenter cohort studies of patients diagnosed with prostate cancer (n = 3705) recruited between 2008–2011, rectal cancer (n = 1215) recruited between 2012–2015, and colon cancer (n = 1891) recruited between 2015–2020. The three studies were registered at isrctn.com/clinicaltrials.gov (ISRCTN06393679, NCT02530593 and NCT01477229). Ethical approvals were obtained from the Regional Ethical Review Boards in Göteborg, Sweden for LAPPRO (Laparoscopic Prostatectomy Robot Open), (EPN 277–07), for QoLiRECT (Quality of Life in Rectal Cancer) in Göteborg, Sweden (EPN 595–11) and Denmark (H-3–2012-FSP26), and for QoLiCOL (Quality of Life in Colon Cancer) in Göteborg, Sweden (EPN 957–14) and Denmark (H-16027323). All patients gave informed consent to participate in the studies. LAPPRO was primarily designed for comparing robot-assisted laparoscopic with open retropubic radical prostatectomy. QoLiRECT and QoLiCOL was designed for exploring patient-reported outcomes after treatment for rectal or colon cancer.
Data on prescriptions of beta-blockers (Anatomic Therapeutic Chemical classification, ATC, code C07) were retrieved from the Swedish Prescribed Drug Register (Läkemedelsregistret) for the period 1 year before and up to 2 years after study inclusion. Information on prescriptions of anti-depressants (ATC code N06A) was also retrieved from the registry. Since we could only retrieve prescription data for Swedish patients the Danish patients in the cohorts were excluded. All three studies collected patient-reported data using a comprehensive questionnaire that was developed from themes identified during patient interviews and subsequently validated by experts and survivors of the respective cancer type. The creation and validation processes for the questionnaires have been previously described in detail [13, 14]. These questionnaires were distributed preoperatively and at 12 months to all patients and at 24 months for prostate and rectal cancer patients. There was no assessment at 24 months in the colon cancer study.
Study designObservational data was used to emulate hypothetical randomized target trials (Additional file 1, Table S1.1). The eligibility criteria of the target analysis were patients diagnosed with prostate, colon, or rectal cancer who had no previous use of beta-blockers. Those who fulfilled eligibility criteria and had an assessment of outcomes (i.e., completed questionnaires) were assigned to one of two strategies.
Strategy 1: Initiate beta-blocker therapy between baseline and follow-up (Active group).
Strategy 2: Refrain from taking beta-blocker therapy between baseline and follow-up (Control group).
The estimands of interest were the ratios (Active vs Control) of odds for poor outcome 12 months after randomization for the endpoints in Table 1, adjusted for baseline values using an intention-to-treat analysis. When estimating the statistical models there is a risk of convergence issues when some response categories of the endpoints have low observed frequencies. To avoid this, categories with very low prevalence were combined prior to statistical analysis.
Table 1 Outcome measures of primary and secondary endpointsThe causal path between initiation of beta-blockers and the outcomes were considered to be confounded by age, self-reported hazardous alcohol consumption, and poor mental health at baseline [15]. To adjust for these variables in the statistical analysis, we emulated a true randomization to the two strategies. Hazardous alcohol consumption was measured by the question “Have you had six glasses or more on the same occasion during the past month?” and categorized as “Yes” if this had happened on at least one occasion. Poor mental health was included as a covariate for all endpoints except for Secondary 1 Depressed mood because the baseline value of this endpoint is highly correlated with mental health. Poor mental health was defined as fulfilling at least one of three criteria: 1) retrieval of a prescription of anti-antidepressants during 12 months before baseline, 2) self-reported as seeking health care due to depression or psychiatric issues, or 3) answered “Yes” or “Don´t know” on the question: “Would you consider yourself depressed?”.
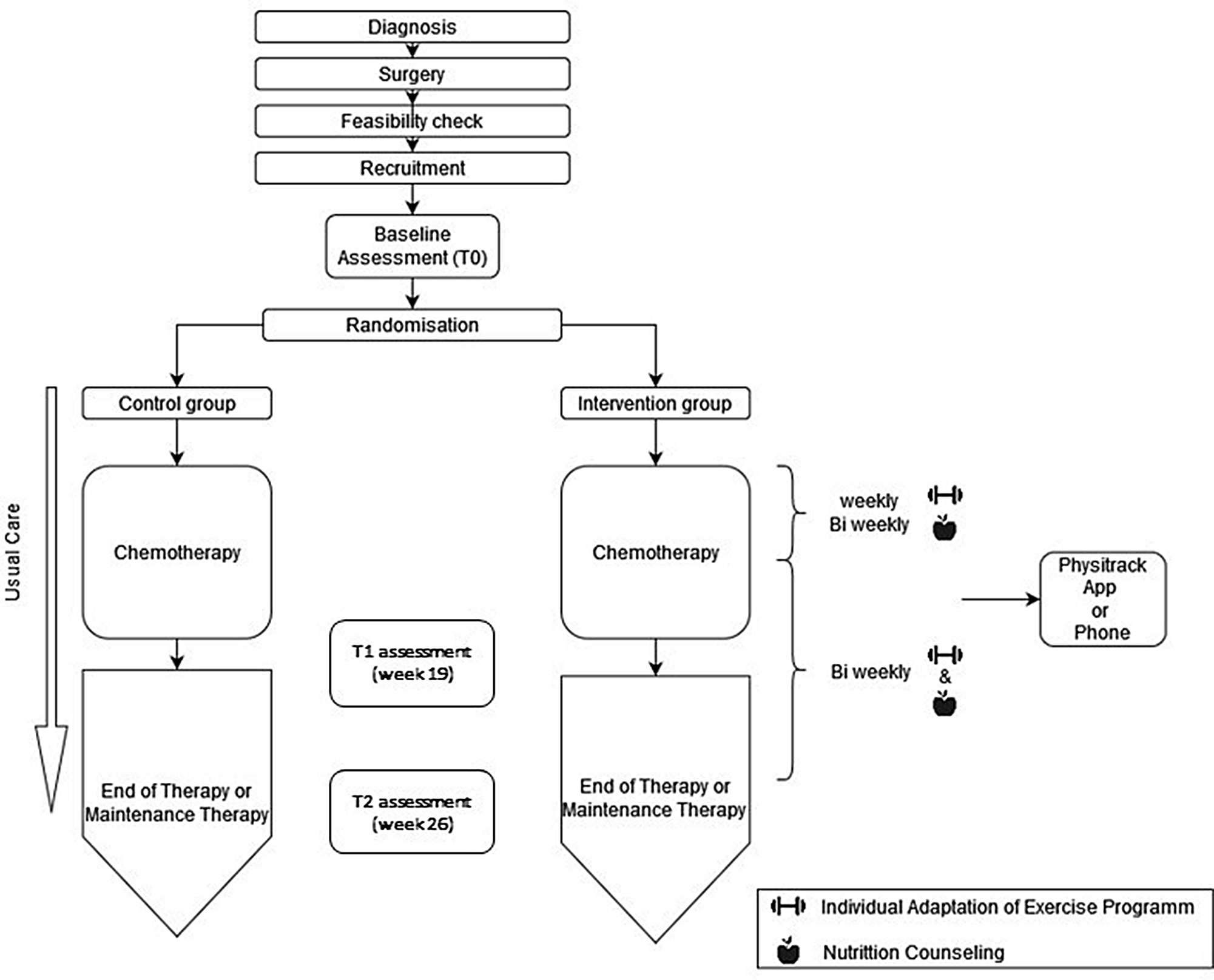
Two trial emulations were performed. In trial 1, the preoperative questionnaire from the cohort studies was used as baseline, and the assessment 12 months after surgery as follow-up. In trial 2, the 12-month questionnaire was used as baseline, and at the assessment at 24 months after surgery as follow-up (Fig. 1). Eligible patients were those who had returned questionnaires to the study secretariat and had no dispensation of beta-blockers in the 12-month period before completing the baseline questionnaire. Given that patients in emulated trials do not necessarily initiate the treatment of interest at time zero (i.e., beta-blockers at baseline), there is a need to incorporate a grace period during which treatment initiation can occur [16]. In this study, the grace period was the entire period of 12 months between baseline and follow-up, during which at least one dispensation of beta-blockers (Active group) or no dispensation at all (Control group) occurred.
Fig. 1
Flow chart of eligible and assigned patients in the emulated trials
Statistical analysesAll endpoints were analysed using a Bayesian ordered logistic regression model with proportional odds [17]. The confounding variables as well as baseline measurements of the respective endpoints were adjusted for by including them as covariates or factors in the analysis, where age was standardized (zero mean and unit variance). The baseline measurement of each endpoint was included in the model as an ordered categorical factor [18]. For the ordered categorical predictor, a Dirichlet prior was used. In the Statistical Analysis Plan (SAP), improper flat priors were prespecified for the intercept and the effects of treatment (Active vs Control) and the adjustment variables of age, binge drinking and signs of poor mental health. However, data sparsity in terms of the low number of patients assigned to the Active group gave rise to convergence issues. Therefore, weakly regularizing priors (Gaussian with zero mean and unit variance on the logit scale) were used in the analysis to ensure convergence of the Markov Chain Monte Carlo (MCMC) samplers. Missing data for endpoints and confounders were handled by multiple imputations (five imputations) using predictive mean matching [19]. Posterior draws were generated for each of the five sub-models using Hamiltonian Monte Carlo Sampling and were subsequently pooled to obtain the final posterior distributions. Results were presented as the posterior means and two-sided 95% credible intervals (CrI) for the odds ratio (OR) from the Bayesian ordered logistic regression model. Higher values (> 1) for the OR mean that patients in the Active group are worse off compared to those in the Control group. Lower values (< 1) mean that patients in the Active group are better off compared to those in the Control group. The posterior predictive distribution across the response categories was also visualized in graphs for each endpoint.
As sensitivity analyses, we performed unadjusted complete case analyses as well as adjusted frequentist analyses where the estimates from the five sub-models were pooled using Rubin’s rules (p. 76) [20]. In addition, analyses were performed of prevalent users of beta-blockers, with dispensation during the 12 months before diagnosis until follow-up. As this analysis does not have a defined time zero and consequently no defined baseline, the analyses were unadjusted. Additional details on the statistical analyses and programming code, results of the sensitivity analyses, convergence diagnostics of the MCMC samplers and characterization of the missing data are presented in the Additional file 1. All data analyses were made in R [21] using the brms [22], mice and MASS [23] packages.
Comments (0)