
Remember me



The prevalence of os trigonum has a large reported range of 1.7% to 50% in the general population1–6 and commonly presents bilaterally.7 The secondary ossification center of the talus fuses with posterior talar body through endochondral ossification into trigonal process or Stieda process between the ages of 7 to 13 years.6,8–10 Otherwise, it will persist as a separate ossicle attached to the posterior talus through a fibrocartilaginous synchondrosis, known as an os trigonum.9,11,12
An os trigonum fracture has been defined as a fracture occurring through the synchondrosis/cartilaginous articulation between the os trigonum and the posterior aspect of the talus. It can also manifest as a fracture through the trigonal process.10,11,13,14 This pathology has a very low prevalence, and bilateral manifestations have not been published before this report.7,10–13 The purpose of this study was to report a case of bilateral os trigonum fractures managed surgically with simultaneous posterior ankle arthroscopic débridement. Written consent for publication of all the data, including the images, was obtained from the patient.
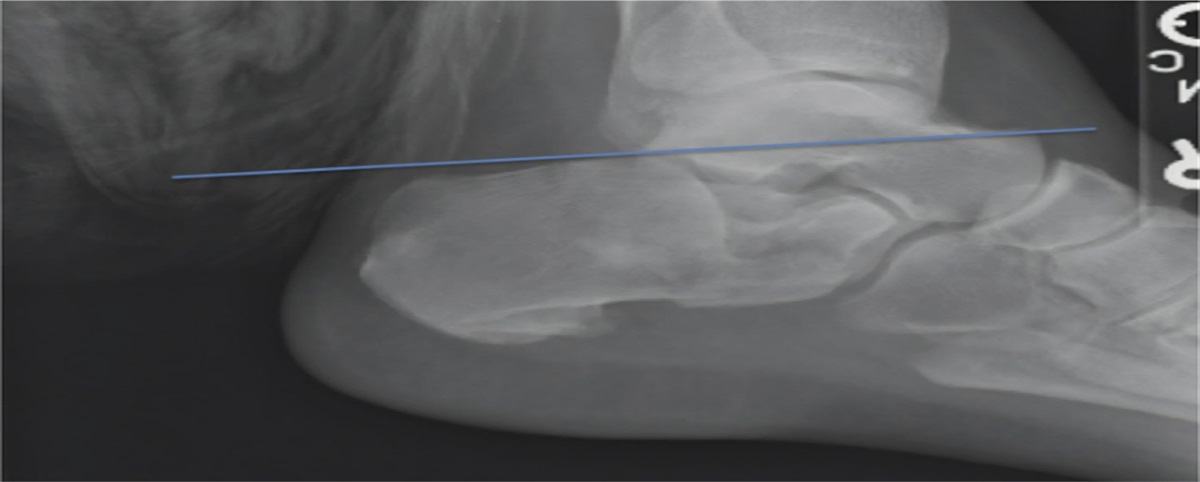
Case ReportA 21-year-old woman presented with 6 weeks of trauma-induced bilateral posterior ankle pain. She had no notable medical history, was 157 cm tall, weighed 52 kg, and had a body mass index of 21.1 kg/m2. Her bilateral ankle injury occurred while jumping from a moving van while wearing 3-inch high heel shoes. She went to a nearby hospital and was diagnosed with bilateral ankle sprains and was immobilized with a short leg cast for 14 days. However, her pain and swelling persisted, and she was unable to walk, necessitating the use of a wheelchair. After 6 weeks, she was referred to our hospital for additional evaluation. Physical examination revealed swelling in both ankles with tenderness at the posterior ankle joint. This pain was aggravated by a jerk test (sudden passive plantar flexion of the ankle). Her active ankle plantar flexion was limited in both ankles because of notable pain. Weakness and decreased muscle mass were also observed. Lateral ankle radiographs showed the presence of an os trigonum/trigonal process in both talus bones, but no fracture lines were detected (Figures 1, A and B and 2, A). Plantar flexion stress radiographs demonstrated the os trigonum to be located between the posterior plafond and the calcaneus in both ankles (Figure 1, C and D). Owing to a strong suspicion of os trigonum injury, CT and MRI scans were obtained, revealing a fracture line through the cartilaginous synchondroses of both os trigonum (Figure 2, B–H) with increased signal intensity in os trigonum in T2-weighted MRI suggestive of bone marrow edema and surrounding fluid accumulation. Because the patient's prior conservative treatment had failed, it was decided to surgically treat the bilateral injury with posterior ankle arthroscopic débridement.
 Figure 1:
Figure 1: Lateral ankle weight-bearing radiographs demonstrating os trigonum bilaterally (A & B, black arrows). Radiographs showing maximum plantar flexion stress test demonstrating pain (nutcracker sign) of the posterior ankle joint (C & D, white arrow).
 Figure 2:
Figure 2: The os trigonum (white arrow, A–H) of the right ankle is demonstrated on a lateral ankle weight-bearing radiograph (A), sagittal CT image (B), axial CT image (C), 3D CT reconstruction image (D), T1-weighted sagittal MRI (E), T2-weighted sagittal MRI (F), T1-weighted axial MRI (G) and T2-weighted axial MRI (H).
Surgical TechniqueThe patient was placed in a prone position with thigh tourniquets under a spinal block. Both feet were placed at the end of the table, and passive dorsiflexion was achieved by leaning of the surgeon's body forward on each forefoot (Figure 3, A). Pertinent anatomical landmarks were then identified and marked (Figure 3, B). Both posteromedial (PM) and posterolateral (PL) portal sites were created at the same height, just medial and lateral, respectively, to the border of the Achilles tendon in line with the inferior tip of the lateral malleolus (Figure 3, B and C).15,16 A blunt dissection of the PM portal was then performed with a straight hemostat oriented toward the third toe (Figure 3, D). The same technique was used in the PL portal and triangulation towards the third toe was done. A 4-mm sheath with a blunt trocar was introduced into the PL portal, followed by a 4-mm 30° arthroscope. A 3.8-mm shaver was then inserted into the PM portal, and triangulation of both instruments was performed until the tip of the shaver was visualized by the arthroscope camera.
 Figure 3:
Figure 3: Photographs showing the patient placed in a prone position with bilateral limb drapes (A). Standard posterolateral (PL) and posteromedial (PM) portals are created at the level of the inferior fibular tip (TF, B), just medial and lateral to the Achilles tendon (TA, B). A camera is introduced in the PL portal, and a shaver is inserted in the PM portal (C). The direction of the shaver should be oriented toward the third toe (D) to prevent injury to medial neurovascular structures (NV, B). C = calcaneus, MM = medial malleolus, TA = Achilles tendon
Soft-tissue débridement was performed using the 3.8-mm shaver (Figure 4, A), creating a working space. The os trigonum was the first osseous structure that could be visualized at this level (Figure 4, B). During the medial débridement, the sharp edge of the shaver should face laterally until the flexor hallucis longus (FHL) was identified (Figure 4, B). The FHL tendon and muscle belly can be confirmed by first metatarsophalangeal joint manipulation and should be used as a medial boundary to protect the neurovascular bundle (Figures 4, B and 5, E). All circumferential soft tissues around os trigonum were then débrided thoroughly using the shaver and arthroscopic scissors. A Freer elevator was then used to identify, mobilize, and free the fractured os trigonum from the posterior aspect of the talus (Figure 4, D and E). Once separated, a grasper or hemostat was used to remove the os trigonum as a whole piece (Figure 4, F and H), or the ossicle can be shaved off by a burr if removal in one piece is unobtainable (left side, Figure 5, C and D). Any prominent edge should be trimmed until no impingement or irritation on the FHL tendon during maximum plantar flexion and dorsiflexion of the great toe was observed (Figures 4, G and 5, E and F). Portals were closed with 3-0 nonabsorbable suture, and soft dressing was applied. Surgical times were 26 and 29 minutes for the left and right ankles, respectively. No intraoperative complications were observed.
 Figure 4:
Figure 4: Images demonstrating the surgical technique of right os trigonum removal (A–H). The intermalleolar septum (IMS) is débrided to provide arthroscopic working space (A). A 3.8-mm shaver is used to débride around the os trigonum with the sharp edge positioned toward the bone and the smooth edge facing the FHL tendon (B). The os trigonum (*, C) of the right ankle is demonstrated, and a Freer elevator can be used to separate the os trigonum from the posterior aspect of the talus (D). The fracture line/cartilaginous articulation can be seen (E, black arrow). The os trigonum is removed using a hemostat (F), and an arthroscopic view of the posterior talus (T) and STJ is demonstrated (G). A gross appearance of the os trigonum after removal is provided (H). * = os trigonum, black arrow = fracture line, C = calcaneus, FHL = flexor hallucis longus tendon, STJ = subtalar joint, T = talus
 Figure 5:
Figure 5: Images demonstrating the surgical technique of left os trigonum débridement (A–F). A 3.8-mm shaver is used to débride around the os trigonum with the sharp edge positioned toward the bone and the smooth edge facing the FHL tendon (A). The os trigonum is demonstrated (*, C), and a 4.0-mm barrel burr is used to shave off the bone in a posterior-to-anterior direction (C & D). Adequate débridement of the os trigonum is verified by performing maximal dorsiflexion (FHL MB is visualized), plantar flexion of the first metatarsophalangeal joint, and with observation of tendon gliding without any impingement of the remaining posterior portion of the talus (E & F). * = os trigonum, C = calcaneus, FHL MB = flexor hallucis longus muscle belly, T = talus
Postoperative RehabilitationThe patient could begin early range-of-motion exercises for the big toe and ankle joint immediately. By the third postoperative day, when she was switched to controlled ankle motion walking boots, she could bear weight as tolerated. By 2 weeks, all stitches were removed, and the boots were replaced with regular tennis shoes. She received instructions to gradually resume all daily activities, perform strengthening exercises for the big toe and ankle joint, and return to her normal studies. She was able to perform double-heel rise at 3 weeks postoperatively (Figure 6). At 6 weeks postoperatively, she was able to engage in noncontact sporting activities such as walking exercises, swimming, and cycling. By 3 months postoperatively, she could participate in all sporting activities with no limitations. Postoperative radiographs are shown in Figure 6.
 Figure 6:
Figure 6: Immediate postoperative weight-bearing lateral ankle radiographs demonstrating bilateral os trigonum/posterolateral process removal (A & B). Photograph of the patient demonstrating a double-heel rise at 3 weeks postoperatively (C). Final postoperative weight-bearing lateral ankle radiographs are shown (D & E).
Functional Outcome MeasurementThe patient completed all preoperative and final postoperative functional outcomes questionnaires (36 months) including visual analog scale, 36-items Short Form survey, and Foot and Ankle Ability Measure. The pain visual analog scale score decreased from 8/10 to 0/10 for both ankles. Significant improvements were noted in the 36-items Short Form survey and Foot and Ankle Ability Measure as summarized in Table 1. No postoperative complications were recorded in this study.
Table 1 - Preoperative and Postoperative Functional Outcomes Functional Outcomes Time Baseline (1st visit) 36 mo Pain VAS 8 0 FAAM (ADL) 2.4 100 FAAM (sport) 0 96 SF-36 (PCS) 26.8 59.3 SF-36 (MCS) 30.3 63.7ADL = activity of daily living, FAAM = Foot and Ankle Ability Measure, MCS = Mental Component Score, PCS = Physical Component Score, SF-36 = 36-items Short Form survey, VAS = visual analog scale
An os trigonum fracture is an uncommon condition17,18; resultantly, only 12 cases have been reported in the literature since 1927 (Table 2).10–13,17,19–21 All previous reports of this trauma were unilateral manifestations, making this study the first documented bilateral case. The mechanism of injury for this pathology is forced hyperplantar flexion that creates compression of the os trigonum by the posterior portion of the tibial plafond and posterosuperior aspect of the calcaneus, earning the nickname “nutcracker syndrome.”22,23 Diagnosis is often challenging, and nondisplaced fractures are usually misdiagnosed as ankle sprains, peroneal tendinitis, or Achilles tendinitis.10,11,19 Therefore, patients with hyperplantar flexion injury history, persistent posterior ankle pain, inability to bear weight,11,13 and reproducible pain on plantar flexion should raise suspicion. A negative radiograph does not rule out the injury, 7,11 necessitating additional investigation with CT and MRI scans.7,13
Table 2 - Demographic Data, Causes, Diagnostic Imaging, Treatment, Outcomes, and Complications of Os Trigonum Fractures Year, Authors No Age Sex Side Cause/Symptom Diagnostic Imaging Associated Fractures Mechanism of Injury Treatment Operation/Approach F/U (mo) Outcomes and Complications 1. 1927, Meisenbach et al17 1 25 M — Squash (sports)/pain and ecchymosis Positive radiograph/free os trigonum No — N/A No surgery 0.5 Able to use foot 2 48 F — Fall (trauma)/pain swelling Positive radiograph/free os trigonum No Dorsiflexion Reduction and using flanged plate No surgery N/A Good results 2. 1975, Lapidus21 3 17 M Lt Football (sports)/pain, ecchymosis, unable to bear weight, limited ROM Negative radiograph/free os trigonum No — Non–weight bearing with crutches No surgery 1 Pain free at 5 wk 3. 1982, Ihle et al10 4 29 M Rt Basketball (sports)/pain, limited ROM, weakness on push-off, crepitus on the posterior ankle Negative radiograph but positive radiograph at 6 mo later/Fused os trigonum No Hyperplantar flexion and inversion Open excision of os trigonum at 6 mo after injury Open posteromedial approach (vertical incision) 12 Full ROM and return to sports at 12 mo 4. 2004 Mouhsine et al7 5 41 M Rt Fall from height (high energy trauma)/pain, unable to bear weight, pain on forced plantar flexion Negative radiograph CT scan positive/free os trigonum No — Non–weight bearing first 2 wk then full weight-bearing short leg cast until 6 wk No surgery 6 Pain free at 6 wk Return to work 7 wk Union at 6 mo 5. 2005, Anwar et al20 6 21 M Lt Soccer (sports)/pain, swelling, limited ROM, unable to bear weight Positive radiograph CT scan positive/fused os trigonum No — Posterior splint 4 d then weight bearing as tolerated developed pain after treatment at 1 yr Open posterolateral approach 3 Almost full range of motion Pain free No functional limitations 6. 2006, Kose et al11 7 32 F Lt Fall down the stairs (trauma)/pain swelling, unable to bear weight, pain on forced plantar flexion Negative radiograph CT scan positive/free os trigonum No Hyperplantar flexion Non–weight bearing short leg cast 3 wk No surgery 15 Asymptomatic Return to normal ADL and sports 7. 2006, Escobedo et al12 8 21 M Rt Motor vehicle accident (high-energy trauma)/pain, swelling, unable to bear weight Positive radiograph CT scan positive/free os trigonum Pelvic, acetabulum, metacarpal, femoral fractures — Immobilization No surgery 2 Union at 2 mo 8. 2011, Uçar et al14 9 21 M Lt Soccer (sports)/pain, swelling Positive radiograph CT scan positive/fused os trigonum No Hyperplantar flexion and inversion Non–weight bearing with crutches 3 wk then full weight bearing No surgery 2 Asymptomatic Union at 2 mo 9. 2016, Yan et al13 10 43 M Lt Soccer (sports)/pain, swelling, unable to bear weight Positive radiograph CT scan positive/free os trigonum No Hyperplantar flexion Non–weight bearing with short leg splint 6 wk No surgery N/A N/A 11 31 M Lt Fall from height (high energy trauma)/pain, swelling, unable to bear weight Positive radiograph CT scan positive/free os trigonum Pilon, lateral malleolus fractures — Ring fixator for pilon fracture No treatment of os trigonum No surgery N/A N/A 10. 2017, Salupo et al19 12 21 M Lt Pole vault athlete (sports)/pain, ecchymosis, unable to bear weight, posterior ankle impingement test positive Negative radiograph MRI positive/free os trigonum No — Excision of os trigonum Open posterolateral approach N/A Return to sports Normal ROM Normal motor power 11. 2020, Rungprai et al 13 21 F Rt Jumping out of the van (trauma)/pain, swelling, unable to bear weight, posterior ankle impingement test positive Negative radiograph MRI positive CT positive/fused os trigonum No Hyperplantar flexion and inversion Débridement of os trigonum Posterior ankle arthroscopy 36 Return to full daily activities and sports VAS 0/10 SF-36 (PCS = 59.3, MCS = 63.7) FAAM (ADL = 100, Sport = 96) No complications 14 21 F Lt Jumping out of the van (trauma)/pain, swelling, unable to bear weight, posterior ankle impingement test positive Negative radiograph MRI positive CT positive/fused os trigonum No Hyperplantar flexion and inversion Débridement of os trigonum Posterior ankle arthroscopy 36 Return to full daily activities and sports VAS 0/10 SF-36 (PCS = 59.3, MCS = 63.7) FAAM (ADL = 100, Sport = 96) No complicationsADL = activity of daily living, FAAM = Foot and Ankle Ability Measure, MCS = Mental Component Score, PCS = Physical Component Score, SF-36 = 36-items Short Form survey, VAS = visual analog scale
Os trigonum fractures can be successfully treated with conservative measures such as immobilization using a short leg cast up to 6 weeks.11–13,24 The success rate is approximately 70%.10–13,17,19–21 Whether osseous union is achieved, it has been proposed that if the patient is asymptomatic, no additional treatment is indicated.25 However, this claim has been disputed by other studies of symptomatic nonunion10,11,20 where associated pain and inflammation have been demonstrated.7,12,20 Therefore, for patients with unresolving symptoms after at least 6 weeks of conservative therapy, surgical treatment should be considered.14,20,26
The standard surgery for os trigonum fracture is an open excision, which can be approached posterolaterally19 or vertically along the midline.10 Although there were no complications identified in our literature review of os trigonum fractures specifically (Table 2), a systematic review of open os trigonum excision using PM (59 patients) and PL (59 patients) approaches reported negative outcomes such as wound and neurological complications at rates between 8% and 21%.27 Posterior ankle arthroscopy has been introduced for the treatment of posterior ankle pathology28 with superior outcomes, decreased soft-tissue injury, less scarring, less postoperative pain, and quicker recovery times.28–30 Using this technique in this report, our patient was able to walk 3 days after her operation, return to full activities of daily living at 2 weeks postoperatively, and resume sporting activities at 12 weeks after treatment. However, experience with this technique and adequate knowledge of posterior ankle anatomy are required to perform this operation safely and effectively.
ConclusionUnilateral os trigonum fractures are rare, and bilateral manifestations are even more uncommon. Patients who present with a history of a hyperplantar flexion injury with persistent ankle pain should raise suspicion for this injury. Negative radiography does not exclude the condition, and CT or MRI studies should be considered. Conservative management is first-line and effective for most cases. In patients with persisting symptoms, posterior ankle arthroscopic débridement demonstrated a notable improvement in functional outcomes, fast recovery times, and low complication rates and could be done simultaneously.
AcknowledgmentsPhinit Phisitkul, MD, Orthopaedic Foot and Ankle Surgeon, Tri-State Specialists, Sioux City, IA, USA. Annunziato Amendola, MD Orthopaedic Foot and Ankle surgeon, Orthopaedic Sports Medicine Surgeon, Duke Ambulatory Surgery Center, Duke University Hospital, Durham, NC, USA. Dr. Phisitkul and Dr. Amendola are mentors for teaching the posterior ankle arthroscopic technique.
References 1. Ahn JH, Kim YC, Kim HY: Arthroscopic versus posterior endoscopic excision of a symptomatic os trigonum: A retrospective cohort study. Am J Sports Med 2013;41:1082-1089. 2. Bizarro AH: On sesamoid and supernumerary bones of the limbs. J Anat 1921;55:256-268. 3. Mann RW, Owsley DW: Os trigonum. Variation of a common accessory ossicle of the talus. J Am Podiatr Med Assoc 1990;80:536-539. 4. Burman MSLP: The functional disturbances caused by the inconstant bones and sesamoids of the foot. Arch Surg 1931;22:936-975. 5. Salyers SGFF: Posterior ankle impingement syndrome in a ballet dancer. Orthop Consult 1989;10:9-12. 6. Zwiers R, Baltes TPA, Opdam KTM, Wiegerinck JI, van Dijk CN: Prevalence of Os trigonum on CT imaging. Foot Ankle Int 2018;39:338-342. 7. Mouhsine E, Djahangiri A, Garofalo R: Fracture of the non fused os trigonum, a rare cause of hindfoot pain. A case report and review of the literature. Chir Organi Mov 2004;89:171-175. 8. Grogan DPWA, Walling AK, Ogden JA: Anatomy of the os trigonum. J Pediatr Orthop 1990;10:618-622. 9. McDougall A: The os trigonum. J Bone Joint Surg Br 1955;37-B:257-265. 10. Ihle CL, Cochran RM: Fracture of the fused os trigonum. Am J Sports Med 1982;10:47-50. 11. Kose O, Okan AN, Durakbasa MO, Emrem K, Islam NC: Fracture of the os trigonum: A case report. J Orthop Surg (Hong Kong) 2006;14:354-356. 12. Escobedo EM, MacDonald TL, Hunter JC: Acute fracture of the os trigonum. Emerg Radiol 2006;13:139-141. 13. Yan YY, Mehta KV, Tan TJ: Fracture of the os trigonum: A report of two cases and review of the literature. Foot Ankle Surg 2016;22:e21-e24. 14. Uçar Bu D, Bozkurt M, Bulut M, Azboy I: Acute fracture of OS trigonum wıth cartilaginous articulation. Int J Med Med Sci 2011;3:89-91. 15. Rungprai C, Phisitkul P, Femino JE, Martin KD, Saltzman CL, Amendola A: Outcomes and complications after open versus posterior arthroscopic subtalar arthrodesis in 121 patients. J Bone Joint Surg Am 2016;98:636-646. 16. Rungprai C, Tennant JN, Phisitkul P: Disorders of the flexor hallucis longus and os trigonum. Clin Sports Med 2015;34:741-759. 17. Meisenbach R: Fracture of os trigonum: Report of two cases. JAMA 1927;89:199-200. 18. Blanchette MA, Grenier JM: Fracture of the lateral tubercle of the posterior talar process caused by a rock-climbing fall: A case report. J Can Chiropr Assoc 2014;58:286-290. 19. Salupo S: Os trigonum fracture: Case report. J Sports Med Allied Health Sci 2017;3:25. 20. Anwar R, Nicholl JE: Non union of a fractured os trigonum. Inj Extra 2005;36:267-270. 21. Lapidus PW: A note on the fracture of os trigonum. Report of a case. Bull Hosp Joint Dis 1975;33:150-154. 22. Uzel M, Cetinus E, Bilgic E, Karaoguz A, Kanber Y: Bilateral os trigonum syndrome associated with bilateral tenosynovitis of the flexor hallucis longus muscle. Foot Ankle Int 2005;26:894-898. 23. Hedrick MR, McBryde AM: McBryde AM: Posterior ankle impingement. Foot Ankle Int 1994;15:2-8. 24. Nyska M, Howard CB, Matan Y, et al.: Fracture of the posterior body of the talus: The hidden fracture. Arch Orthop Trauma Surg 1998;117:114-117. 25. Chao W: Os trigonum. Foot Ankle Clin. 2004;9:787-796. 26. Hamilton WG, Geppert MJ, Thompson FM: Pain in the posterior aspect of the ankle in dancers. Differential diagnosis and operative treatment. J Bone Joint Surg Am 1996;78:1491-1500. 27. Zwiers R, Wiegerinck JI, Murawski CD, Smyth NA, Kennedy JG, van Dijk CN: Surgical treatment for posterior ankle impingement. Arthroscopy 2013;29:1263-1270. 28. van Dijk CN, Scholten PE, Krips R: A 2-portal endoscopic approach for diagnosis and treatment of posterior ankle pathology. Arthroscopy 2000;16:871-876. 29. Guo QW, Hu YL, Jiao C, Ao YF, Tian DX: Open versus endoscopic excision of a symptomatic os trigonum: A comparative study of 41 cases. Arthroscopy 2010;26:384-390. 30. Weiss WM, Sanders EJ, Crates JM, Barber FA: Arthroscopic excision of a symptomatic Os trigonum. Arthroscopy 2015;31:2082-2088.
Comments (0)