We treated two patients with mCRPC who achieved a response for more than 12 months with PARPi treatment. Both cases had not only BRCA2 loss but also RB1 variants (splice site variant or loss), and these double variants are known to lead to an aggressive phenotype with a epithelial to mesenchymal transition [4]. BRCA2 loss may be less likely to cause reversion mutation, one of the mechanisms of PARPi resistance [5], and the two cases in this study are predicted to have long-term response to PARPi treatment. A recent report showed that PCa organoids harboring a heterozygous co-deletion of BRCA2 and RB1 alleles exhibited depletion of both BRCA2 and RB1 proteins, suggesting that heterozygous loss leads to haploinsufficiency of these proteins. Since the RB1 variant (NM_000321.3:c.2489 + 1G > C) has been reported to disrupt the canonical splice site, potentially leading to aberrant splicing and either an abnormal protein or a transcript subject to nonsense-mediated mRNA decay, a similar process might have occurred in our case 1, resulting to co-deletion of BRCA2 and RB1 alleles. PCa with BRCA2 loss and concomitant RB1 co-loss has been reported as more sensitive to PARPi treatment than that with BRCA2 loss alone [6]. This may be another reason why PARPi was effective in the long term in these two cases of BRCA2 and RB1 double variants. Although several BRCA2 and RB1 co-loss cases had been reported [7,8,9,10], to our knowledge, only one report showed the efficacy of PARPi (veliparib) in patients with mCRPC with BRCA2 and RB1 co-loss [7], as in our case (Table 1). However, Taza F et al. reported that PARPi were effective in 11 of 19 mCRPC patients with co-mutation of RB1 and BRCA2, whereas PARPi were effective in 53 of 80 mCRPC patients without RB1 but with BRCA2 mutation[11].
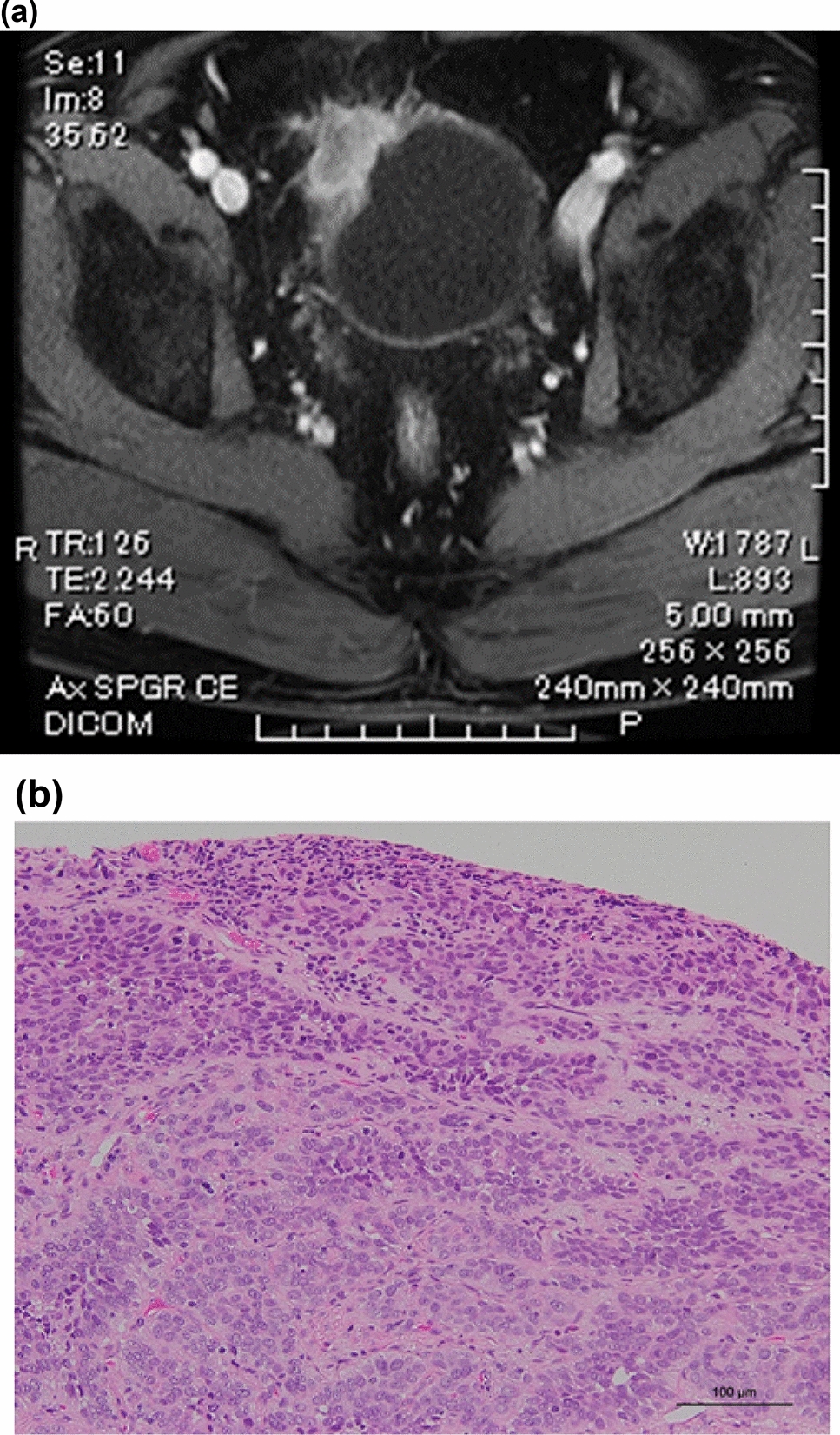
Table 1 Case reports of PCa with BRCA2 and RB1 variantsAccording to the ClinVar Database (https://www.ncbi.nlm.nih.gov/clinvar), the RB1 variant (NM_000321.3:c.2489 + 1G > C) has been previously reported to result in a splice variant, potentially causing intron inclusion between exons 23 and 24. However, based on the COSMIC Database (https://cancer.sanger.ac.uk/cosmic), the amino acid change is unknown (Genomic Mutation ID: COSV57300119). The RB1 variant (NM_000321.3:c.2489 + 1G > C) has been reported as a somatic variant in only one patient with metastatic PCa [12]. To check if the RB1 variant resulted in RB1 protein loss as indicated in the previous report, we performed immunostaining for RB1, which was negative in lung resection specimens.
In case 2, besides BRCA2 loss, biallelic RB1 loss and TP53 variant were present. The co-loss of TP53 and RB1 is known as one of the features of neuroendocrine prostate cancer, resulting in decreased AR expression and increased neuroendocrine marker expression[13]. Iwasawa et al. reported that BRCA2 alteration was found only in the TP53 and RB1 altered CRPC cases without neuroendocrine differentiation[10]. In case 2, similarly, AR expression was low but neuroendocrine markers, e.g. chromogranin A and synaptophysin, were completely not stained by immunostaining.
Among BRCA2 variants of PCa, biallelic homozygous deletions are common. Sokol et al. reported that 28.9% (176/609) of BRCA2 variants of PCa were biallelic homozygous deletions (shown in Supplementary Table of Ref [14]). Both heterozygous and homozygous BRCA2 losses had poor prognosis with non-PARPi treatment [15]. Conversely, patients with mCRPC with BRCA2 homozygous deletion had superior rPFS and overall outcomes with PARPi treatment, suggesting that, in these tumors, PARPi resistance may be harder to develop [16].
In addition, there are two interesting aspects of these two cases. First, the two cases had IDCP genomic characteristics with distinct genomic profiles of somatic variants (ERG rearrangement, the loss or variants of RB1, TP53, and PTEN, as well as MYC amplification) and BRCA2 variants [17]. Second, both cases had low serum PSA levels at the time of mCRPC, which may indicate the presence of pathogenic variants of RB1 and/or TP53 [18].
This report has several limitations. First, the mechanism of biallelic somatic BRCA2 loss has not yet been elucidated. Second, it is not clear whether the RB1 splicing variant in Case 1 is identical to RB1 loss. Third, treatment with the PARPi olaparib is ongoing and it is not clear how long the therapeutic effect will continue.
In conclusion, these two cases of Japanese patients with mCRPC suggest that PARPi may be effective in the long term in patients with BRCA2 and RB1 double pathogenic variants. Further analysis is needed to evaluate if the presence of RB1 mutation can be a predictive biomarker for the efficacy of PARPi in patients with BRCA-mutated mCRPC.









Comments (0)