
Remember me

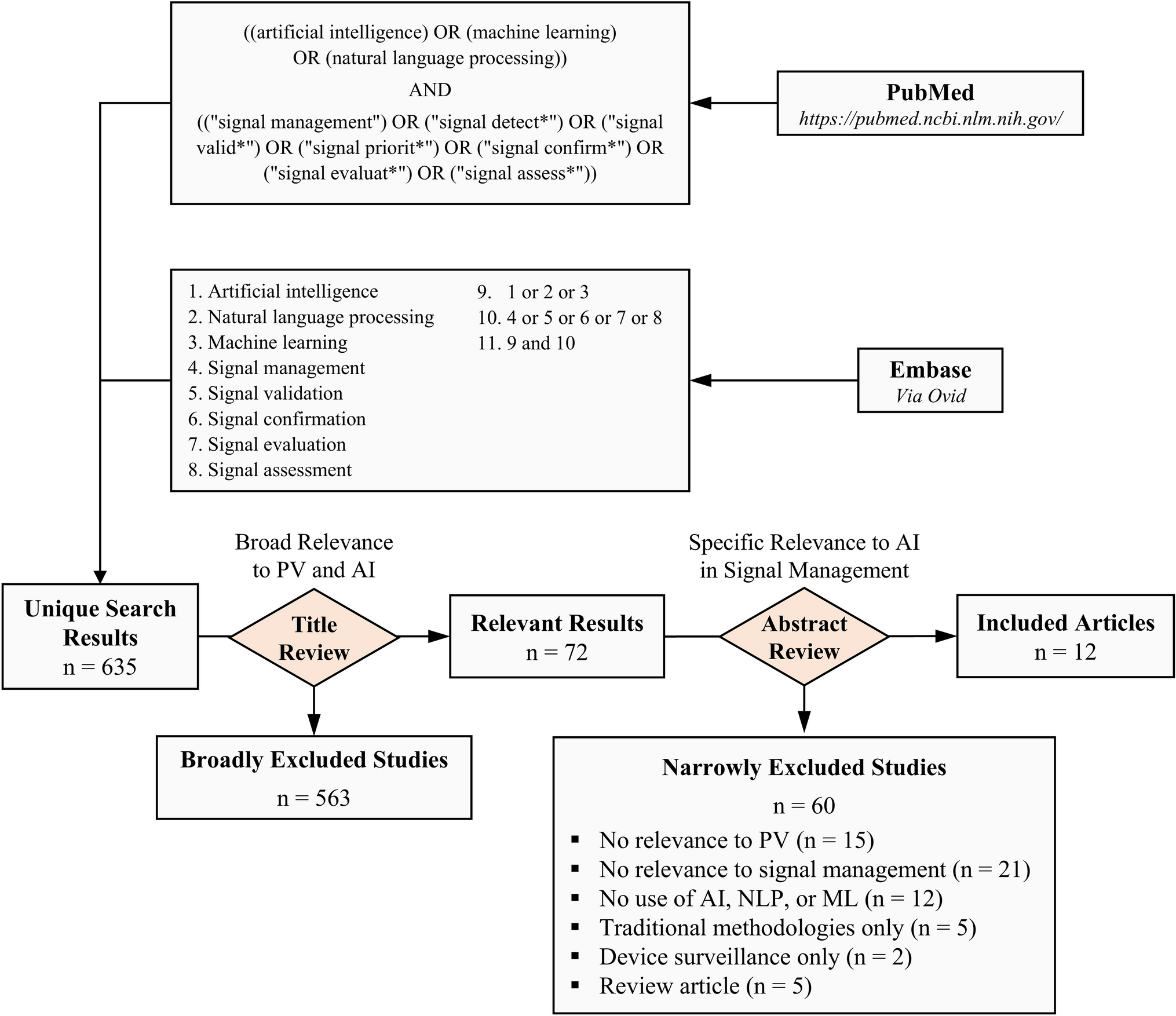

The search in PubMed and Embase yielded a total of 1617 records (Fig. 1). Upon removal of duplicates, 1047 records with potential relevance were identified for further screening. Following an independent screening process based on title and abstract, a total of 70 articles was assessed for further eligibility. In total, 20 articles were excluded for the following reasons: only abstract available (n = 7), no relevant information on mitigation strategies (n = 11), no access to full text (n = 1), and insufficiently described methodology (n = 1). In the end, 50 articles were included from the PubMed and Embase search. An additional 10 articles were included through the snowballing method, resulting in a total of 60 included articles in this review.
Fig. 1
PRISMA flow diagram: identification, review, and selection of articles included in the systematic review
3.1 Characteristics of Included StudiesThe descriptive characteristics of the 60 studies included in this review are presented in Table 1 by country, type of study, type of intervention, therapeutic area, and its funding source. Most of the studies were conducted in Europe (58%, 35/60), followed by Oceania (17%, 10/60), North America (12%, 7/60), and Eurasia (3%, 2/60). For the remaining six studies, the country in which the study was conducted was not specified. The majority (93%, 56/60) of the studies consisted of original research (interventional or observational study or qualitative research). Of these, 44 studies (73%) followed an interventional study design (RCTs mainly and one non-randomised study), nine had an observational study design (cross-sectional, case study and cohort), and the remaining three studies were qualitative research studies. In total, four literature reviews were included (two systematic literature reviews, and two non-systematic literature reviews). In approximately half (48%, 29/60) of the studies, a pharmacological intervention was reported, while for one-third (38%, 23/60) of the studies a non-pharmacological intervention (e.g., transcranial direct-current stimulation, electro-cutaneous pain stimuli) was reported as the type of intervention. One study (2%) employed both a pharmacological and nonpharmacological intervention, while the remaining seven (12%) did not report an intervention type, as these were systematic or (non-) systematic literature reviews or qualitative research studies. Among 28 studies that reported a pharmacological intervention, seven (12%) specifically mentioned the use of a biosimilar, whereas the remaining studies (35%, 21/60) reported other pharmacological interventions. Ten (17%) of 60 reviewed studies were conducted within the context of biosimilar switching. Approximately one-third of the reviewed studies (30%, 18/60) were conducted within the field of pain research, followed by rheumatology (13%, 8/60) and oncology (7%, 4/60). Other areas of interest (22%, 13/60) included acupuncture, respiratory diseases and osteopathy. Considering the studies for which any funding was mentioned, funding was by the public sector only (50%, 30/60) (i.e., university grant, research foundation or a government authority), except for two (3%) studies which were funded by the private sector (i.e., pharmaceutical industry).
Table 1 Descriptive summary of the studies included in the systematic review3.2 Quality AppraisalThe quality of the included studies was assessed using the following three tools: MMAT (56 studies), JBI Critical Appraisal Checklist for Systematic Reviews and Research Syntheses (two studies), and SANRA (two studies). All of the included studies that underwent methodological quality assessment were rated as ‘high’ quality, except for four [57,58,59,60], which were assessed using the MMAT criteria. Of these four, three RCTs [58,59,60] were categorised as ‘medium’ quality, and one qualitative study [57] was categorised as ‘low’ quality. For all three RCTs, it was insufficient to judge how randomisation was (appropriately) performed, and outcome assessors were not blinded to the intervention. For the qualitative study, sources of bias included inadequate description of data collection methods to address the specific research questions, lack of clarity on how the findings were adequately derived from the data, insufficient substantiation by the data for interpretation of the findings, and lack of coherence between data sources, collection, analysis and interpretation.
3.3 Overview of Identified Mitigation Strategies Within and Outside the Biosimilar ContextIn this review (n = 60 articles), 15 distinct mitigation strategies for the nocebo effect were identified. Of these, five strategies were solely identified in the biosimilar context, three strategies were solely identified outside the biosimilar switching context (non-biosimilar context), and seven strategies were identified both within and outside the biosimilar context. An overview of these strategies is shown in Table 2 with a definition or description of each strategy, the context in which the strategy was identified and an example of how the strategy could be applied in the context of biosimilar switching. It is important to acknowledge that some overlap exists between certain mitigation strategies. The main reason for this categorisation approach is to ensure consistency when classifying all identified studies based on their primary mitigation strategy(ies) employed in each study.
Table 2 Overview of identified mitigation strategies for the nocebo effect3.4 Studies on Mitigation Strategies Within the Biosimilar-Switching ContextIn Table 3, a summary of the main characteristics of the included studies within the biosimilar switching context is presented.
Table 3 Summary of the main characteristics of the included studies within the biosimilar switching context3.4.1 Quantitative StudiesIn total, seven quantitative studies within the biosimilar switching context evaluated mitigation strategies for the nocebo effect. These included five observational (cohort) studies [33, 35, 45, 61, 62], one randomised controlled trial [63] and one nonrandomised controlled trial [64].
a.Shared decision-making strategy
Five studies employed a shared decision-making strategy by incorporating the patients in the process, but varying outcomes in retention rates [33, 35, 45, 61, 64]. Among these five studies, four studies utilised an opt-in transition method in which patients actively agreed to the transition [33, 45, 61, 64]. Only one study utilised an opt-out transition method (i.e., transitioning patients to the biosimilar unless they actively object) [35]. In the study by Boone et al, the authors utilised shared decision making with an opt-in transition method as a single mitigation strategy [33]. No significant differences in effectiveness were found between the originator and biosimilar infliximab for inflammatory bowel disease and rheumatology patients after transitioning. However, an overall nocebo response rate of 12.8% was measured among patients who switched to the biosimilar. While the study was not controlled to measure the impact of a shared decision-making strategy on the nocebo effect, the authors hypothesised that employing such strategy could potentially reduce the occurrence of the nocebo effect.
b.Shared decision-making strategy combined with other strategies
Four studies employed shared decision making in combination with other mitigation strategies [35, 61, 64, 65]. In the study by Scherlinger et al, physicians provided uniform information (verbally) about biosimilars to patients with rheumatic disease in a confident way alongside employing a shared decision making with an opt-in transition method [65]. Furthermore, a telephone interview was proposed after the initial consultation, which included a standardised set of open and closed questions related to their social-cultural background, fears and beliefs, and adherence to treatments and other medical interventions. A retention rate of 72% was reported after switching patients from originator to biosimilar infliximab, which was significantly lower than that in their two control cohorts and a historic cohort. Furthermore, nearly half of the patients who transitioned back to the originator showed no worsening of disease activity score, suggesting a reluctance to the switch despite their initial agreement. Despite initially agreeing, two patients refused to switch due to receiving contradictory and negative information by their regular pharmacist. Patients who refused to switch also showed a statistical trend towards older age, longer disease duration and a long history of originator (etanercept) use. Müskens et al. utilised an opt-in transition method alongside educating HCPs about biosimilars and using supporting material through a standardised letter to inform patients about biosimilars and the transition process [61]. The authors found a significantly lower one-year retention rate for patients treated with etanercept (outpatient setting) in the transition cohort compared to the historical cohort (73% vs 89%) and attributed this to the nocebo effect. After adjusting for the latter, comparable retention rates were found for both the transition and historical cohorts. The authors concluded that a shared decision-making approach with an opt-in option may not be sufficient as strategy to mitigate for the nocebo effect compared to a more directive opt-out approach [61]. In a second study by Tweehuysen et al, the authors adopted for an enhanced communication strategy [35]. This approach involved a shared decision making with an opt-out transition method, enhanced treatment information (proper provision of patient information in case of objective or subjective health complains), and education about the nocebo effect alongside soft-skills training to HCPs. Over six months, a treatment persistence rate of 90% was found for patients with rheumatic disease who switched to biosimilar etanercept, compared to 92% for the originator etanercept. The acceptance rate of the biosimilar was also higher than that reported for CT-P13 in their first transitioning study. The authors concluded that an enhanced communication strategy, together with more experience and the absence of group-think effects with fellow patients (e.g., viewing the biosimilar as inferior and encouraging each other to restart therapy with the originator biologic) resulted in higher acceptance and persistence rates following open-label shared decision making transitioning to biosimilars [35].
c.Taking a multidisciplinary approach
In four studies, the significance of a multidisciplinary team approach in biosimilar switching was highlighted [35, 62, 64, 66]. Levivien et al, evaluated the impact of consultations with a clinical pharmacist before seeing a rheumatologist [64]. Their focus was on patient education about biosimilarity and involving them in the decision process, particularly in choosing between a pen or pre-filled syringe. The authors concluded that a consultation with a clinical pharmacist showed a significant positive impact on the switch rate to biosimilar adalimumab or etanercept (69.4% vs 41.1% in the control group), but not on the nocebo effect since the percentage of patients still on biosimilar after a one-year follow-up was lower in the intervention group (72.5%) compared to the control group (81.3%). Petit et al, employed a tailored communication strategy by a multidisciplinary team [62]. This strategy involved (i) providing training of the physicians and nurses on biosimilars and the nocebo effect, (ii) a prominent role for nurses as the first point of contact in announcing the switch, providing switch information to the patients (e.g., simple sentence mentioning change of name), and answering questions that emerged according to the pre-determined semantic tools (i.e., vocabulary to be used to inform about biosimilars) and patient's needs, (iii) using a consistent vocabulary (one voice principle), (iv) providing written supporting information to patients upon their request (focusing on the similarity between the biosimilar and the originator), and (v) soft-skills training to HCPs, including motivational communication, enabling them to offer interviews to patients if needed. The biosimilar retention rate was higher than three other European non-switch cohorts’ retention rates and no significant difference was found in the retention rate (91.2% vs 96.2%) from that for the historical (non-switch) cohort. The authors concluded that a multidisciplinary tailored communication strategy focusing on establishing a relationship of trust between the nurses and patients can minimise the nocebo effect.
d.Positive attribute framing
In one experimental study conducted by Gasteiger et al, patients with rheumatic disease received video explanations by a physician, which employed positive attribute framing by simply emphasising the similarities between the originator biologic and biosimilar rather than differences alongside positive body language and verbal cues (e.g., nodding and smiling) [63]. The authors found that positive framing led to patients being approximately 2.4 times more willing to switch to a biosimilar infliximab and reported significantly higher perceived efficacy of biosimilars compared to patients in the control group.
3.4.2 Qualitative StudiesThree qualitative studies proposed mitigating strategies for the nocebo effect within the biosimilar switching context. Study designs included one semi-structured interview study [67], one report of a stakeholder workshop [57], and one non-systematic literature review [68].
a.Communication strategies (open, empathic, validating communication and positive framing)
All three studies emphasised the importance of communication strategies including positive communication or framing and empathic communication to mitigate the nocebo effect [57, 67, 68]. Barbier et al, reported the following communication mitigation strategies: (i) HCP communication with a focus on International Non-Proprietary Names (ii) transparent and honest communication and (iii) using positive verbal and non-verbal suggestions to inform the patient about the reasons for the switch and highlighting that the biosimilar is equally safe and effective [67]. Empathic communication strategies providing reassurance, showing empathy, and empowering patients, and utilising soft skills, were identified as well as equally important [68]. One study also emphasised the significance of using a validating communication strategy, which extends beyond just showing empathy. It is more about the act of communicating acceptance and understanding [57].
b.Education and training of health care professionals about biosimilars, the nocebo effect, and soft skills
Two studies also discussed that adequate education should be provided to the HCP team about biosimilarity and the nocebo effect, explaining reasons behind the switch and how to switch, so that they in turn are well-equipped to transfer correct information to the patients [57, 67]. In addition, one study highlighted the important of soft skills training to HCPs [68].
c.Taking a multidisciplinary approach
Two studies highlighted the importance of multidisciplinary team involvement to include physicians, nurses, pharmacists, psychologists and patients, in the switch process [57, 67]. The central role of nurses in patient education and communication about biosimilars was highlighted in the study by D’Amico et al. [57]. Nurses can provide personalised information about biosimilars tailored to each individual patient based on their risk profile for the nocebo effect, educational background and age [57].
d.Shared decision-making strategy
One study identified the importance of a shared decision-making process, which involves both the patient and the physician actively contributing to the decision making of a treatment and where the patient is fully aware of this treatment choice [57].
e.Providing personalised and supporting information
The value of providing tailored information considering each patient’s needs was identified in two studies [67, 68]. The latter refers to providing understandable and concise information and recognising patients with many risk-factors for nocebo effects and allocating more time for counselling and education about the nocebo effect for those patients [67, 68]. In addition, supporting information should be understandable, readable, concise, and in patient’s mother tongue [67].
f.Organisational aspects of the switch
Barbier et al, emphasised that prior to the actual switch, a structured switch plan should be set up as well as organising the switch moment and providing a follow-up moment with the patient. The structured switch plan should be set up as a multi-stakeholder project with assigned responsibilities [67]. Clear and transparent communication with patients is also important and should cover the reasons behind the switch, the safety and efficacy of the biosimilar, and any practical implications for patients. Furthermore, the switch moments should be planned over time, ensuring that not all patients are switched simultaneously. Lastly, regular follow-up moments should be planned with patients to address any concerns or AEs.
3.5 Studies on Mitigation Strategies Outside the Biosimilar ContextTable S6 and S7 provide a summary of the main characteristics of the included quantitative and qualitative studies, respectively, which were conducted in various fields outside the biosimilar switching context.
3.5.1 Quantitative StudiesQuantitative studies outside the biosimilar switching context mainly included interventional studies (84%, 42/50), followed by observational studies (8%, 4/50). All interventional studies consisted of a RCT study design. The observational studies comprised three cohort studies and one cross-sectional study. Primary outcomes measures that were reported often included pain–pain intensity, pain severity, pain expectancy (30%, 14/46), number of reported side effects (28%, 13/46), and headache occurrence, headache frequency and maximum headache level (7%, 3/46).
a.Positive attribute framing
The most common mitigation strategy was positive communication or positive framing, which was employed as a single strategy by half of the studies (50%, 25/50) outside biosimilar switching context. Of these, most studies (52%, 13/25) reported significant evidence that nocebo effects can be minimised by providing positive communication or positive framing (in either verbal or written form) about treatment-related side effects [59, 69,70,71,72,73,74,
Comments (0)