
Remember me





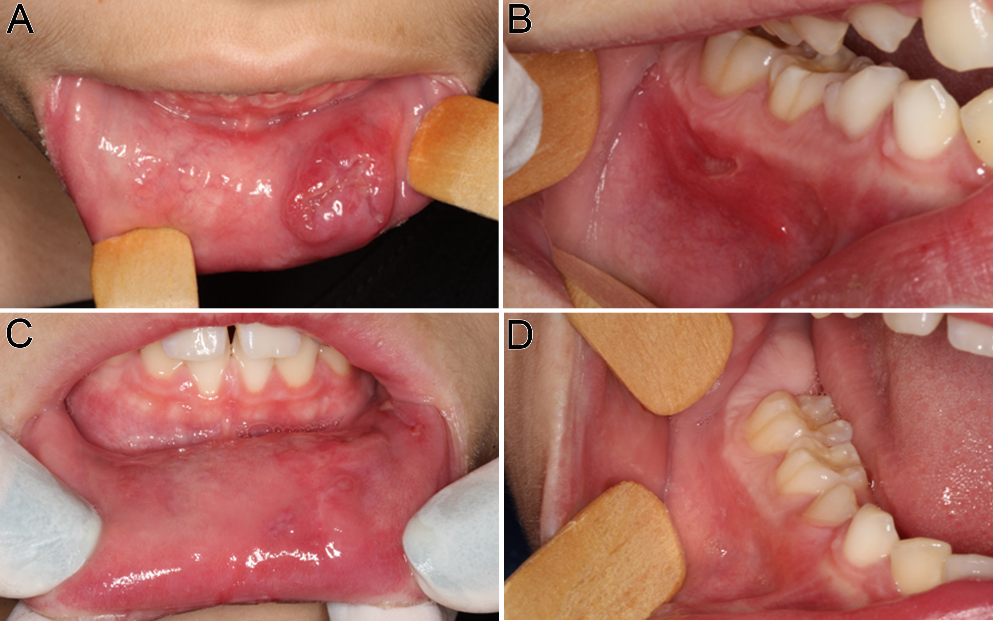
The 74-year-old man presented with a progressively enlarging ulcer on the posterior aspect of right-sided upper gingiva and edentulous ridge of maxilla (#15 and #16 area) (Fig. 1A), accompanied with pain for several months. No symptoms of mast cell activation syndrome, such as fever, flushing, or diarrhea, were observed. The patient reported no significant past medical, personal, or family history. On physical examination, no palpable neck lymphadenopathy was noted.
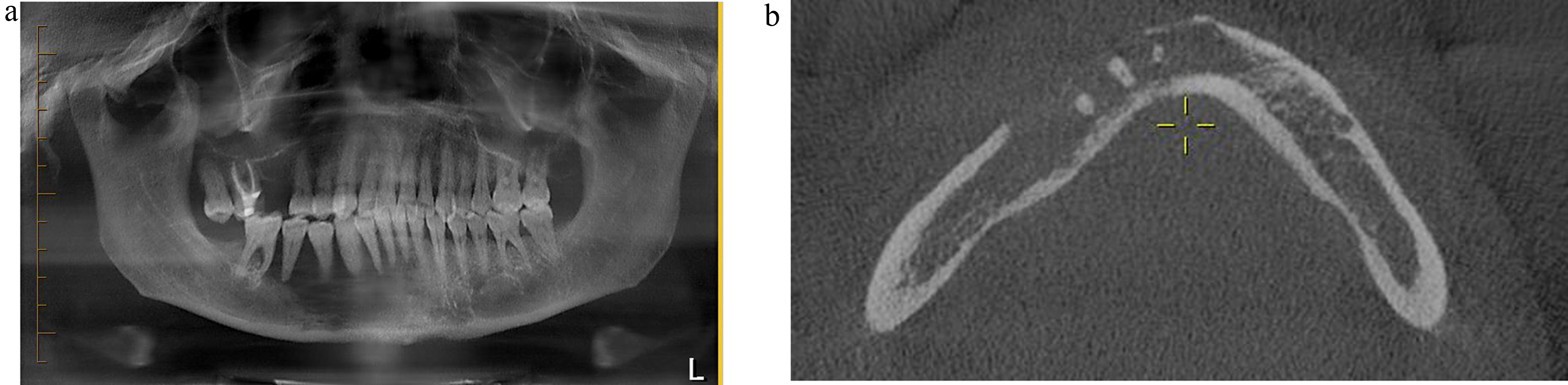
Fig. 1
Clinical presentation. (A) Intraoral view showing redness and swelling of the gingival mass with ulceration in the posterior portion. (B) Coronal magnetic resonance T1-weighted image with contrast enhancement showed a right maxillary mass
Laboratory tests revealed mild to moderate anemia (Hb = 11.3 g/dL, HCT = 33.2%, MCV = 95.4 fL, and MCH = 32.5 pg) and mild leukopenia (WBC = 3,500 per µL). Blood levels of absolute neutrophil count (ANC) (2251 per µL), eosinophils (1.2% of circulating leukocytes), basophils (0.3% of circulating leukocytes), platelet count (PLT = 186,000 per µL), serum tryptase (3.6 ng/mL, reference range ≤ 11), and lactate dehydrogenase (LDH) (172 U/L, reference range ≤ 250) were normal.
The magnetic resonance imaging (Fig. 1B) of the head and neck region, performed after the administration of intravenous contrast material, revealed a tumor measuring up to 3.4 cm in diameter on the floor of the right maxillary sinus, with associated bone destruction. Subsequent positron emission tomography identified a tumor in the right upper gum (standardized uptake value [SUV] of 5.7, score 4) and a right paratracheal nodal lesion (score 2). Abdominal ultrasonography showed no hepatomegaly or splenomegaly.
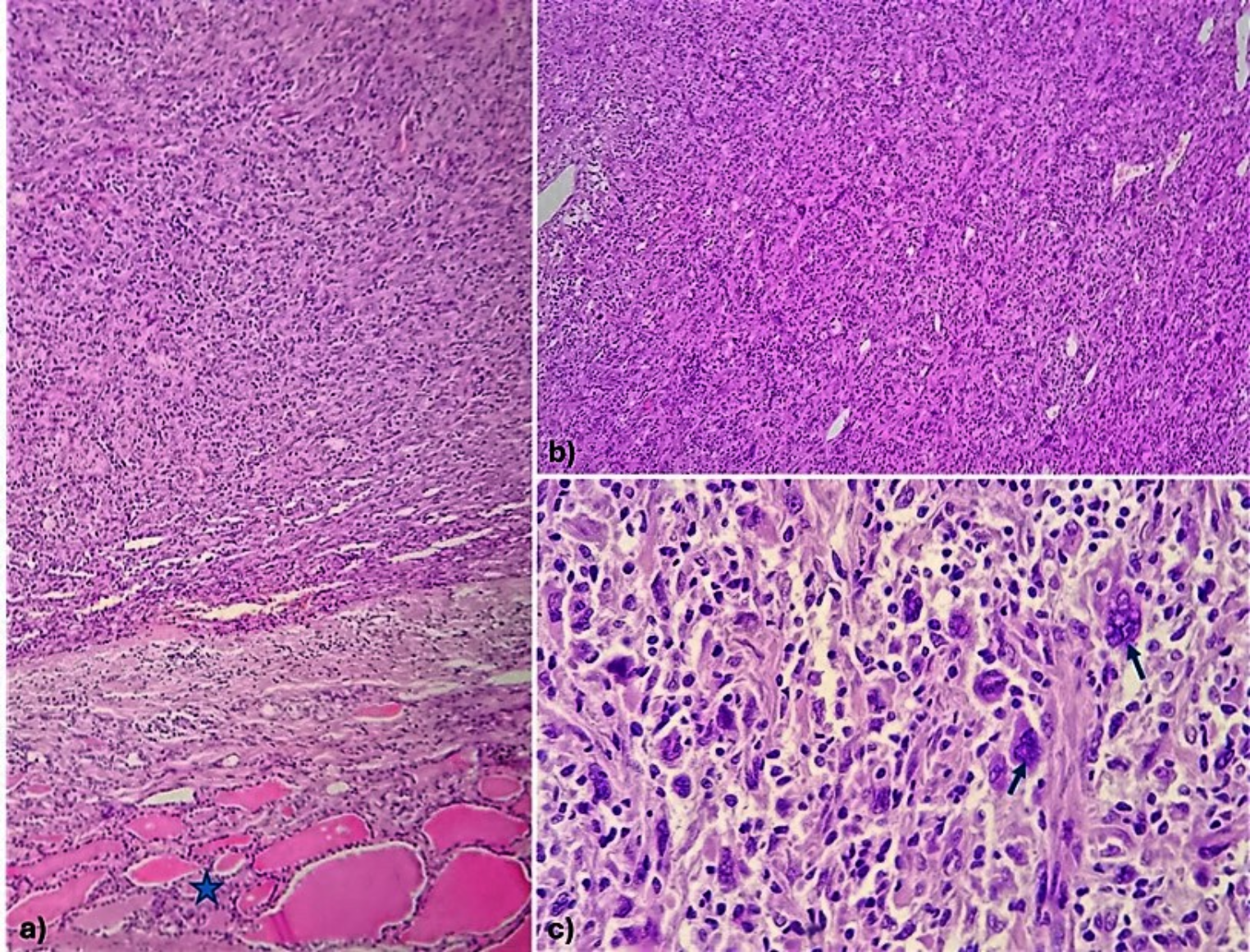
Pathological FindingsA wide excision (inferior maxillectomy) and right-sided neck dissection (levels I to III) were performed. Gross examination of the excised tissue revealed an infiltrative white tumor measuring 2.8 × 2.5 × 2.2 cm, invading the maxilla. Histologic examination showed a subepithelial tumor composed of monotonous medium-sized round cells with oval nuclei, vesicular to finely granular chromatin, inconspicuous to punctate nucleoli, and ample eosinophilic to pale cytoplasm, arranged in diffuse solid sheets with an intervening vascular network (Fig. 2A and C). Mild to moderate pleomorphism was observed, along with rare multinucleated giant cells (Fig. 2D). No spindle cells or eosinophil aggregation were present. Frequent mitoses were noted (> 10/10 high-power fields). The tumor infiltrated the stroma, blood vessels, nerve bundles, trabecular bone, and atrophic minor salivary glands without apparent desmoplastic reaction (Fig. 2B). The overlying squamous epithelium showed no dysplasia or tumor involvement. All dissected lymph nodes were free of malignancy.
Fig. 2
Histopathologic features of mast cell sarcoma affecting the gingiva and the maxillary sinus. (A) A low-power photomicrograph depicted the subepithelial tumor cells and the overlying stratified squamous epithelium (H&E, 100X). (B) A medium-power photomicrograph showed the infiltrating neoplastic cells and the atrophic minor salivary glands (H&E, 200X). (C) A high-power photomicrograph revealed a proliferation of monomorphic tumor cells with oval nuclei, indistinct to punctate nucleoli, eosinophilic-granular to pale cytoplasm, and brisk mitoses (H&E, 400X). (D) Rare multinucleated giant tumor cells were also observed (H&E, 400X)
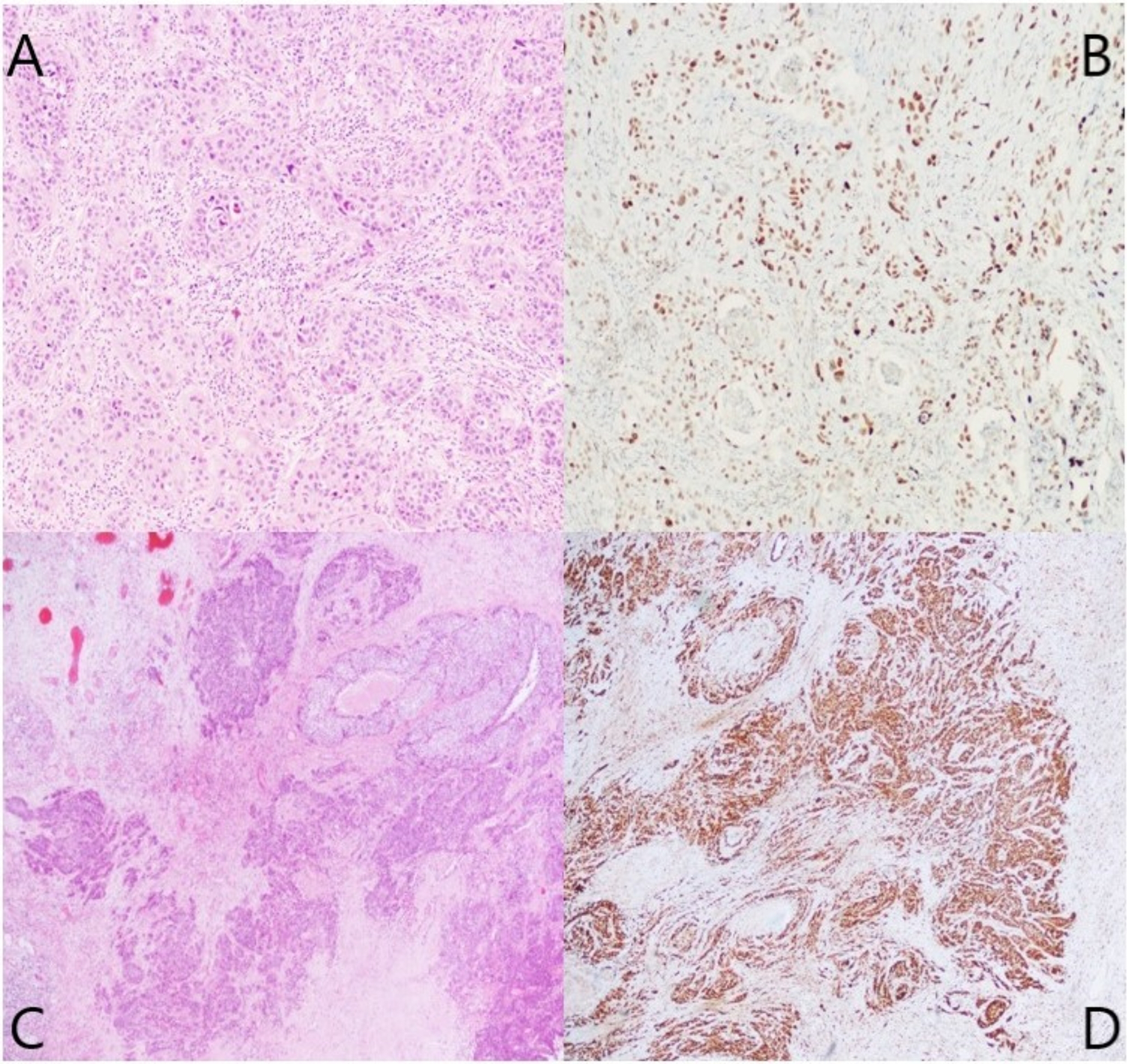
A panel of immunohistochemical stains was initially performed. Tumor cells were negative for epithelial markers AE1/AE3 and CAM5.2, and also negative for p40, NUT, chromogranin, desmin, NKX2.2, S100, SOX10, HMB45, GATA3, CD45 (LCA), CD3, and CD20, with intact INI1 and BRG1 nuclear expression. They demonstrated patchy, moderate to strong positivity for INSM1 and synaptophysin (Fig. 3E-F).
Fig. 3
Immunohistochemical stains showed that the neoplastic mast cells expressed (A) CD117, (B) mast cell tryptase, (C) CD33, (D) CD43, (E) INSM1, and (F) synaptophysin (all in 400X)
While excluding most common sinonasal undifferentiated neoplasms, the H&E morphology suggested consideration of hematologic neoplasms despite negative expression for CD45 (LCA), CD3, and CD20. Additional immunohistochemical stains were performed. The tumor cells were negative for CD25, myeloperoxidase (MPO), CD34, CD123, CD138, and CD163 but strongly positive for CD117, CD13, and CD33 (Fig. 3A and C) and focally positive for mast cell tryptase, CD30, CD43, and CD68 (Fig. 3B and D). KIT mutation analysis was negative for the p.D816V mutation. These histomorphologic and immunophenotypic findings were consistent with those of a mast cell sarcoma.
Subsequent bone marrow aspirate, trephine biopsy, and flow cytometry study were performed after the pathologic diagnosis. The bone marrow aspirate smear (Fig. 4A) showed numerous immature mast cells, accounting for 70% of total marrow elements, with variably sized nuclei, occasionally lobulated (type II hypogranular atypical mast cells), an increased nuclear-cytoplasmic ratio, and basophilic granules in the cytoplasm. The bone marrow biopsy (Fig. 4B) revealed sheets of neoplastic cells occupying over 60% of marrow space, characterized by oval nuclei, moderate eosinophilic to pale cytoplasm, and frequent mitoses. Immunohistochemistry revealed positivity for CD117, mast cell tryptase (Fig. 4C and D), and CD30, and negativity for CD2, CD25, CD34, and MPO. Flow cytometry of the bone marrow confirmed expression of CD117, CD13, and CD33. These findings supported the diagnosis of mast cell leukemia.
Fig. 4
The subsequent bone marrow aspirate smear (A) and trephine biopsy (B) revealed dense infiltrates composed of more than 20% hypogranular atypical mast cells, type II, which were positive for CD117 (C) and mast cell tryptase (D), consistent with mast cell leukemia (A, Liu stain, 1000X; B, H&E, 400X; C-D, 400X)
Follow-up InformationLow-dose chemotherapy with vincristine and methotrexate was administered. However, pancytopenia progressed and jaundice (direct bilirubin = 8.9 mg/dL) developed 2 months after diagnosis. Magnetic resonance cholangiopancreatography revealed newly formed multiple liver nodules and a splenic nodule, suggesting possible disease progression. The treatment was shifted to high-dose chemotherapy with cytarabine. Unfortunately, the patient experienced respiratory failure and died three months after the initial diagnosis.
Comments (0)