
Remember me




Unlike GB tumors, the proportion of benign tumors in EHBD accounts for only 6% [38], and CCA, IPNB, neuroendocrine neoplasm (NEN), amputating neuroma (AN), and biliary sludge, etc., should be differentiated. Furthermore, diagnosis of lateral spreading and depth invasion are also important.
As described in the morphological classification, BDPLs can be broadly classified into papillary and nodular types (Fig. 9). According to a clinicopathological study of CCA, the incidence of superficial spreading, which is continuous with the main tumor and extends ≥ 20 mm into the mucosal epithelium, was 25.0% in distal CCA and 11.1% in perihilar CCA (p < 0.0001) [20]. Furthermore, the frequency of superficial spreading differs greatly depending on the gross type, and its incidence was 46.5% in the papillary type and 12.2% in the nodular type (p < 0.0001) [20]. Therefore, classification of BDPLs into papillary and nodular types is useful not only for the differential diagnosis but also for the diagnosis of tumor extension (Table 2).
Table 2 Characteristics of papillary-type and nodular-type CCAEchogenicityCCA can be predominantly hypoechoic or hyperechoic or have mixed echogenicity depending on the amount of internal fibrosis, mucin, and calcification. However, nodular-type CCA tends to show heterogeneous hypoechoic to isoechoic echogenicity compared with the liver parenchyma (Fig. 13). On the other hand, papillary-type CCA (Fig. 14) and IPNB tend to show homogeneous hyperechoic to isoechoic echogenicity [18, 19], which may be due to the scattering and reflection of ultrasound.
Fig. 13
Nodular-type CCA. US shows a hypoechoic lesion with a nodular surface (↓) in the perihilar BD (a). EUS depicts the discontinuity of the OHL (←), suggesting tumor invasion beyond the subserosa (b). Peroral cholangioscopy shows a flat elevated nodular-type CCA (*) (c, d)
Fig. 14
Papillary-type CCA. US shows a hyperechoic polypoid lesion in the hepatic duct (↓) (a) and also depicts the papillary pattern of the mucosal surface (↓), reflecting lateral tumor spreading around the main tumor (b). Peroral cholangioscopy shows a papillary-type CCA (*) (c) and its lateral spreading (←) on NBI mode (d)
Biliary NEN is a rare tumor that is supposed to arise from Kulchitsky cells and mostly shows heterogeneous hypoechoic echogenicity [39,40,41,42]. AN is also a rare tumor, usually arising from a remnant cystic duct after cholecystectomy, and shows homogeneous hypoechoic echogenicity [43,44,45,46,47,48]. Biliary sludge usually shows hyperechoic to isoechoic echogenicity with dotted hyperechoic spots.
Surface contourPapillary-type CCA often exhibits papillary to lobular surface structures (Fig. 14). Nodular-type CCA often presents with obstructive jaundice at the time of onset, making it difficult to evaluate the surface contour of the main lesion. However, when the surface characteristics of the hepatic extension are included, the lesion often presents as nodular with an irregular surface. On the other hand, papillary or cauliflower-shaped tumors in the expanded BD are the characteristic feature of IPNB (Fig. 15). However, it is sometimes difficult to assess the surface contour of IPNB in cases with mucus.
Fig. 15
IPNB. A high-frequency transducer shows a hyperechoic to isoechoic polypoid lesion in the hepatic duct and also depicts an inner hypoechoic layer, reflecting superficial spreading (↓). (a Right subcostal longitudinal scan, b right subcostal transverse scan)
NEN usually shows a round shape with a smooth contour [40,41,42] and may resemble a submucosal tumor with a capsule [40, 42]. AN also shows a well-defined elevated submucosal tumor-like appearance with a thin normal cystic duct epithelium on cholangioscopy [46]. Both EUS and IDUS also show oval tumors with a smooth surface [43,44,45,46,47], and a hyperechoic rim on the surface is recognized in some cases [45, 46]. In contrast, biliary sludge is characterized by changes in shape and surface contour associated with positional changes.
Mucosal surface around BDPLs (diagnosis of lateral spreading)Superficial intraductal spreading is a characteristic feature of CCA [49] (Figs. 14, 15), and can be used for differential diagnosis. According to a clinicopathologic study, the frequency of superficial spreading (extending ≥ 20 mm into the mucosal epithelium) was 46.5% in the papillary type and 12.2% in the nodular type (p < 0.0001) [20].
According to an EUS study, irregularities of the IHL and/or inner hypoechoic layer reflected superficial spreading, and EUS diagnosed intraepithelial (mucosal) spreading in 52.9% of cases [50]. IDUS findings of irregularity of the mucosal surface and/or uneven or localized thickening of the IHL of the BD adjacent to the main tumor were also used in the diagnosis, and the sensitivity, specificity, and accuracy of the longitudinal extent of cancer on the hepatic and duodenal sides were 82%, 70%, and 78% and 85%, 43%, and 70%, respectively [51]. Tamada et al. reported that a papillary pattern of the BD mucosal surface and heterogeneous BD wall thickening (width 1.8 mm) with irregular outer marginal or asymmetric BD wall thickening (width 1.8 mm) with a rigid inner edge on IDUS may be signs of longitudinal spreading of CCA [52]. In studies on GB carcinoma (GBC), US, especially with a high-frequency transducer with zoom magnification, could detect slight localized thickening of the inner hypoechoic layer around GBC, which corresponds to lateral spreading of flat-type GBCs [53, 54].
Therefore, localized thickening of the internal hypoechoic layer and the papillary pattern of the mucosal surface reflect lateral tumor spreading, suggesting CCA. Since Tamada et al. emphasized the importance of asymmetrical BD wall thickening as the finding of longitudinal tumor spread [55], short-axis images of the BD are more important than long-axis images for the evaluation of lateral extension.
Vertical layer structure of BDPLs (diagnosis of depth invasion)As mentioned above, when employing high-frequency transducers, the BD wall structure can be identified in two or three layers: an IHL and an OHL, or an IHL, a middle hypoechoic layer, and an OHL. Here the description is divided into IHL and OHL.
Characteristics of the innermost hyperechoic layer (IHL)According to studies of the GB wall, the source of the IHL is considered mostly interface echoes [22], and also include the mucosa [23]. Since BD NEN [40, 42] and AN [44, 46] are often covered by nonneoplastic mucosa and resemble a submucosal tumor, the IHL may be recognized in those cases.
Irregularity or discontinuity of the wall layer structureBecause tumor invasion into the adipose layer of the subserosa causes irregularity of the OHL, and tumor invasion beyond the subserosa causes disruption of the OHL, both irregularity and discontinuity of the OHL suggest wall thickening due to malignancy. However, the inner hypoechoic layer contains not only the mucosa and muscularis propria but also the fibrous layer of the subserosa [21], and an intact OHL suggests not only a benign lesion but also CCA with tumor invasion within the fibrous layer of the subserosa.
Since the muscularis propria of EHBD is thin, short-axis images with magnified images using a high-frequency transducer are strongly recommended to evaluate the irregularity or discontinuity of the wall layer (Fig. 16).
Fig. 16
Discontinuity of OHL of nodular-type CCA. Although the long-axis image using a high-frequency transducer shows the discontinuity of the OHL (↓) and an inner hypoechoic layer, reflecting superficial spreading (a), the short-axis image shows the discontinuity of the OHL (↓) more clearly (b)
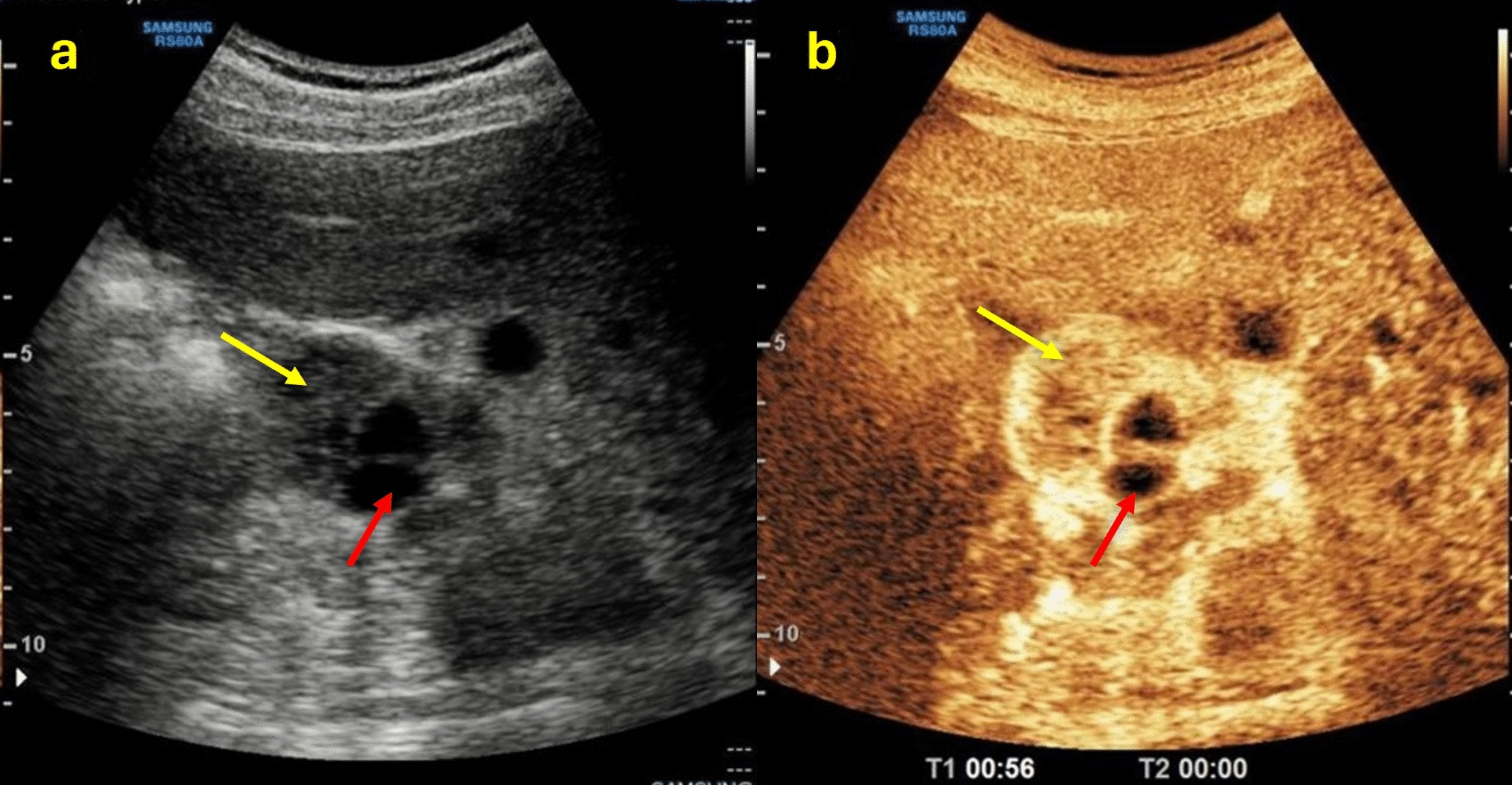
Contrast‑enhanced US (CEUS)According to Fontán et al. [56], CEUS demonstrated early enhancement and posterior washout in CCA. The sensitivity, specificity, positive predictive value, and negative predictive value of CEUS were 85.7%, 88.2%, 94.7%, and 71.4%, respectively. Xu et al. [57] studied the dynamic behavior of hilar CCA using CEUS, demonstrating hyperenhancement, isoenhancement, and hypoenhancement in the arterial phase in 43.8%, 43.8%, and 12.6%, respectively, and 93.8% of the cases presented washout in the portal and late phases.
The papillary or solid components of IPNB showed scarce (80%) or rich (20%) blood supply on color Doppler US [18]. On CEUS, however, they showed homogeneous hyperenhancement (92.3%) or isoenhancement (7.7%) in the arterial phase and hypoenhancement during the portal and late phases [18]. CEUS may facilitate the diagnosis of IPNB and exclude the possibility of sludge, mucus, or blood clots because they are not enhanced. AN is usually hypervascular [44,45,46] and uniformly enhanced at an early phase [44]. The essential contribution of CEUS at this time is differentiation among tumors and non-enhanced material, including lithiasis without acoustic shadow, blood clots, and debris [18, 36, 56]. CEUS is also useful for ruling out concomitant malignant tumors in cases with filling stone or biliary sludge.
From the above, because CCA is the most common lesion among BDPLs, it is important to diagnose tumor extension and depth invasion in addition to the differential diagnosis. Nodular-type CCA is usually hypoechoic and is more likely to invade vertically. In contrast, papillary-type CCA is often hyperechoic and tends to extend laterally. Both irregularity and discontinuity of the OHL suggest tumor invasion beyond the fibrous layer of the subserosa. Slight localized thickening of the inner hypoechoic layer and a papillary pattern on the mucosal surface around BDPLs may suggest lateral spreading of CCA.
Comments (0)