
Remember me






This prospective study was conducted at the Orthopedics and Traumatology Clinic of Düzce University Faculty of Medicine. It included 30 patients diagnosed with plantar fasciitis (PF) following clinical examination and investigations, excluding other potential causes of heel pain. Patients were included if they had been symptomatic for at least 12 months and had not responded to conservative treatments, and were over 18 years old. The patients were divided into two groups: the PRFA group (n = 17), which underwent pulse radiofrequency ablation, and the surgical group (CR group, n = 13), which underwent open plantar fascia release surgery. Detailed information about the study’s purpose, procedure, duration, potential complications, and possible problems were provided to all participants Patients were randomly assigned to the treatment groups without considering smoking status. Ethical approval for the study was obtained from the Ethics Committee of Düzce University Faculty of Medicine on March 26, 2023, with decision number 2023/43.
Inclusion criteria for the study were: patients over 18 years of age with symptoms for at least 12 months, diagnosed with plantar fasciitis through clinical and radiographic differential diagnosis, and unresponsive to first-line exercises, standard insoles, and non-steroidal anti-inflammatory treatment. Exclusion criteria included previous heel surgery, steroid injection into the heel within the last three months, history of heel trauma, allergic reactions to anesthetic agents, bone anomalies in the knee and ankle, local infections, presence of a pacemaker, peripheral neuropathy, and malignancy.
Patients presenting to the clinic with heel pain, diagnosed with PF through history and physical examination, symptomatic for at least 12 months, and unresponsive to at least six months of conservative treatments (exercise, standard insoles, NSAIDs, ESWT, and local steroid injections) were evaluated. Detailed examinations were performed, and differential diagnoses were made using radiographs, MRI, CT scans, blood tests, and other investigations as needed. Sociodemographic characteristics and complaints of the patients were recorded. Hemogram and biochemical tests were performed, and lateral and anterior-posterior foot radiographs were taken. Patients were advised to continue their standard exercise programs and refrain from using NSAIDs during the study period. Clinical evaluations were conducted preoperatively and postoperatively at three months, six months, and one year, using the Foot Function Index (FFI), American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot score, Visual Analog Scale (VAS), and Roles-Maudsley Score (RMS), along with lateral and anterior-posterior foot radiographs.
Clinical evaluation methodsFoot function index (FFI)The FFI is a commonly used self-report form that measures the impact of foot pathologies on pain, disability, and activity limitation. Patients rate their pain on a scale from 0 (no pain) to 10 (worst possible pain) across three sections: pain, disability, and activity limitation. Each section is scored and averaged to a total score out of 100, with higher scores indicating greater pain, disability, and activity limitation [13].
American orthopaedic foot & ankle society (AOFAS) scoreThis score evaluates functional outcomes objectively, including pain (40 points), limitations in activities (50 points), walking distance and gait abnormalities, range of motion, and stability of the foot (10 points). Scores range from 0 to 100, with 91–100 considered excellent, 81–90 good, 71–80 fair, and 70 and below poor [14].
Visual analog scale (VAS)The VAS is a simple and widely used method for assessing pain intensity. Patients rate their pain on a scale from 0 (no pain) to 10 (worst possible pain). In this study, patients evaluated their pain at rest, during the first step in the morning, and during exercise [15].
Roles-maudsley score (RMS)The RMS is a practical and reliable method for assessing pain and its relationship with activity. It is easy to understand for patients and is rated on a four-point scale: (1) no pain during all activities (excellent result), (2) occasional discomfort during all activities (good result), (3) pain after prolonged activity (fair result), and (4) pain limiting daily activities (poor result) [16].
Radiological evaluation methodsCalcaneal pitch angleThe angle between a line drawn parallel to the inferior cortex of the calcaneus and a line drawn from the lowest point of the calcaneus to the lowest point of the fifth metatarsal head. This angle reflects the inclination of the calcaneus relative to the horizontal plane, with a normal value of 21–29 degrees. It decreases in equinus and increases in calcaneus deformity [17].
Meary’s angleThe angle between the long axis of the talus and the long axis of the first metatarsal. This angle indicates the alignment of the forefoot relative to the hindfoot, with a normal range of -4° to + 4°. Angles of 4–15 degrees indicate mild, 15–40 degrees moderate, and over 40 degrees severe pes planus [18].
Hibbs angleThe angle between the longitudinal axis of the first metatarsal and the longitudinal axis of the calcaneus, normally 130–160 degrees [19].
AP talus-first metatarsal angleThe angle between the long axis of the talus and the long axis of the first metatarsal, normally ranging from − 5 to + 5 degrees [20].
AP talocalcaneal angle (kite angle)The angle between the long axis of the talus and the long axis of the calcaneus, with a normal range of 15–30 degrees [20].
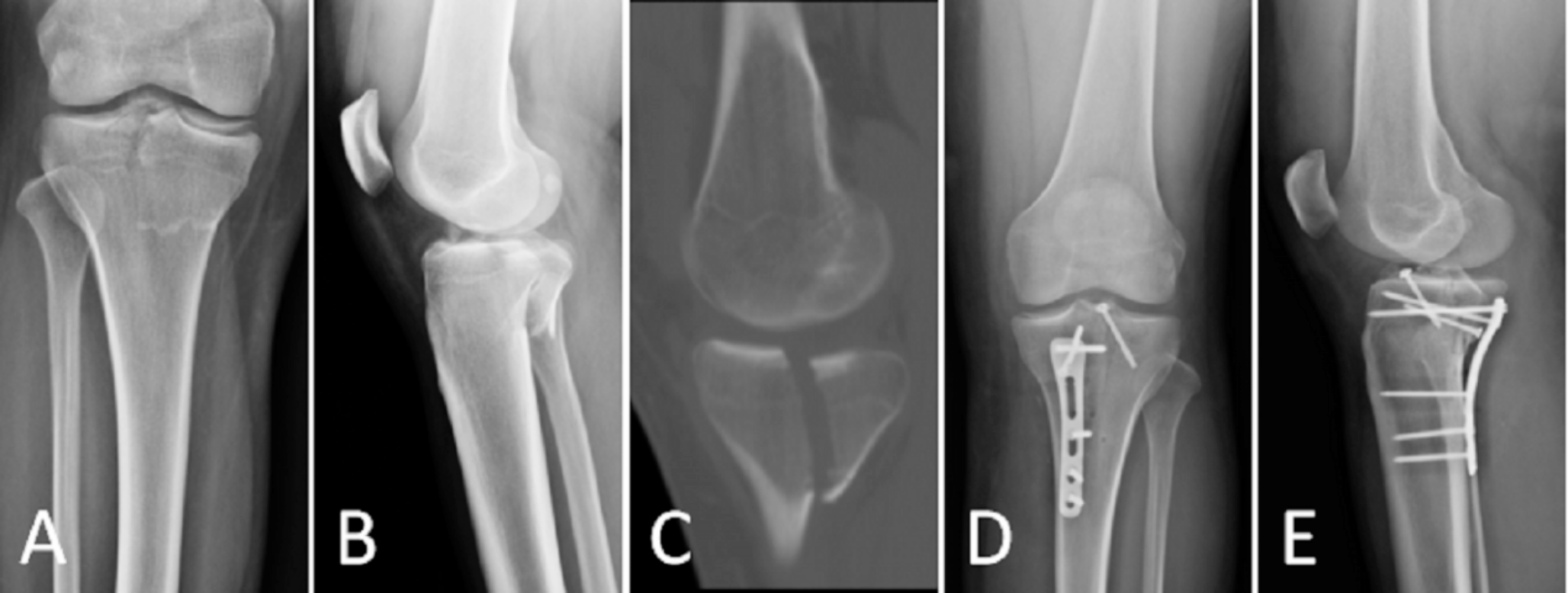
Treatment methodsPulse radiofrequency ablation (PRFA)Procedures were performed in the operating room at Duzce University Faculty of Medicine. Patients were marked at the service, and a grounding pad was placed on the calf of the treated extremity. A hypodermic cannula with a stylet was inserted through the skin to the anteromedial calcaneus. The stylet was removed, and an electrode was placed. Using the COOLIEF radiofrequency device, simulation mode was activated, and current was gradually increased from 0 to 1 V to determine the sensory threshold. If the threshold was above 1 V, the application area was adjusted. Sensory response was confirmed at voltages below 0.5 volts. Motor control was conducted at 2 Hz, with no involuntary contractions indicating proper placement. PRFA was applied at 42 °C for eight minutes at 20 m/s intervals, aiming for an impedance of 250–500 ohms. After the procedure, 1 ml of 5 mg bupivacaine was injected to prevent pain during nerve ablation (Fig. 1) [21].
Fig. 1
Stages of pulsed radiofrequency ablation. A: Placement of the grounding pad B: Application of hypodermic cannula with a stylet C: Removal of the stylet needle and insertion of the electrode D: Application of radiofrequency E: Administration of anesthetic substance after the procedure
Open plantar aponeurosis releaseProcedures were performed in the operating room with the patient under spinal anaesthesia. The affected extremity was positioned laterally, sterilized, and draped. A 3 cm incision was made medially from the heel, and approximately 40% of the plantar fascia was released. The wound was irrigated, a drain was placed, and the incision was sutured and dressed (Fig. 2) [22].
Fig. 2
Stages of plantar fascia release surgery. A: Sterilization of the operation site B: Patient position and view after covering with sterile drapes C: Identification of the incision area with fluoroscopy D: Display of the incision area E: Exposure and release of the plantar fascia F: Placement of the drain and skin closure
Statistical analysisStatistical analyses were performed using NCSS 2007 Statistical Software (Utah, USA). Descriptive statistical methods (mean, standard deviation, median, interquartile range) were used, along with the Shapiro–Wilk normality test. Independent t-tests compared normally distributed variables, Friedman tests for multiple time comparisons, Dunn’s multiple comparison tests for subgroup comparisons, Wilcoxon tests for paired time comparisons, Mann Whitney U tests for non-normally distributed variables, and chi-square tests for categorical data. Results were considered significant at p < 0.05.
Comments (0)