
Remember me



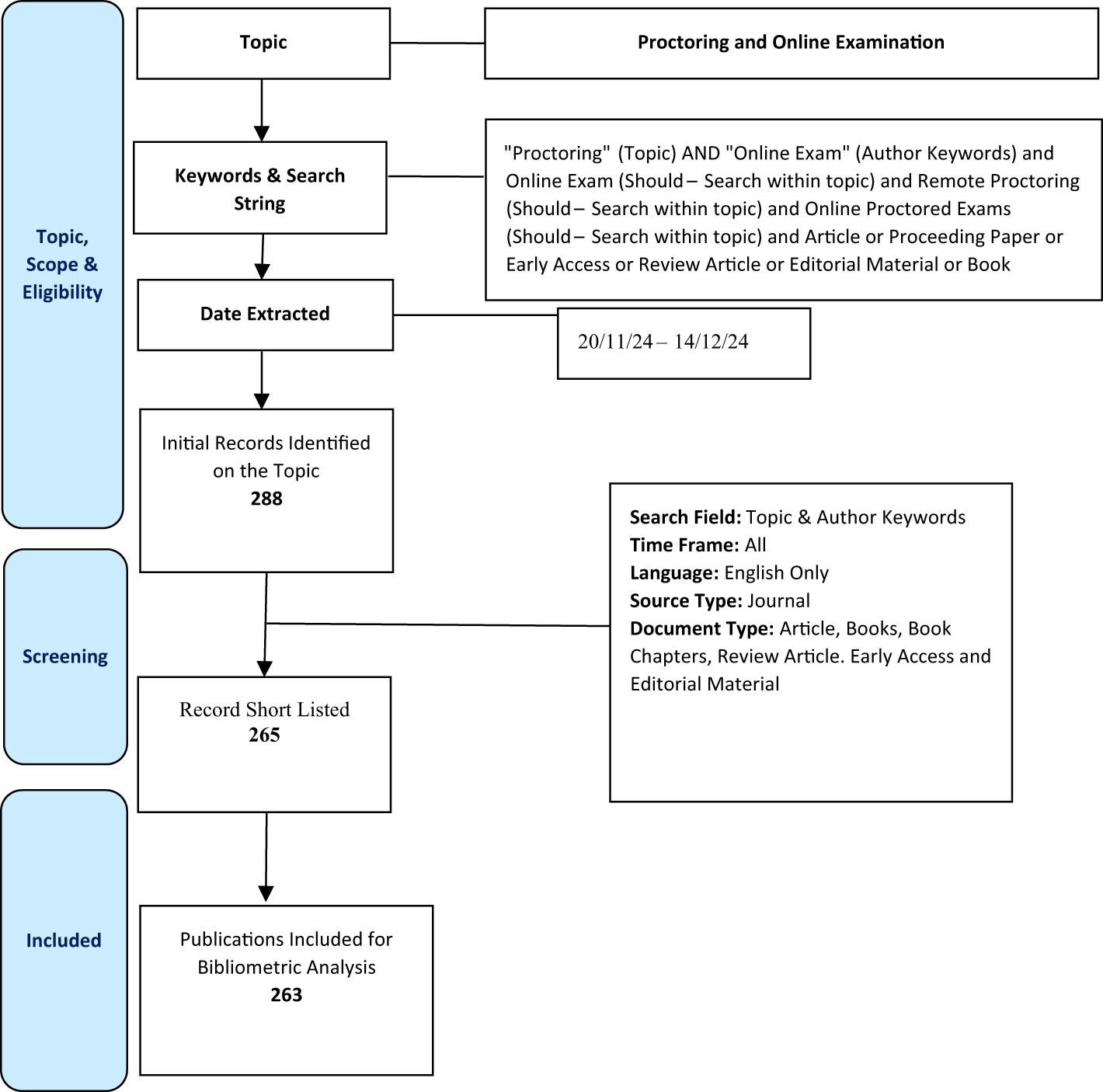
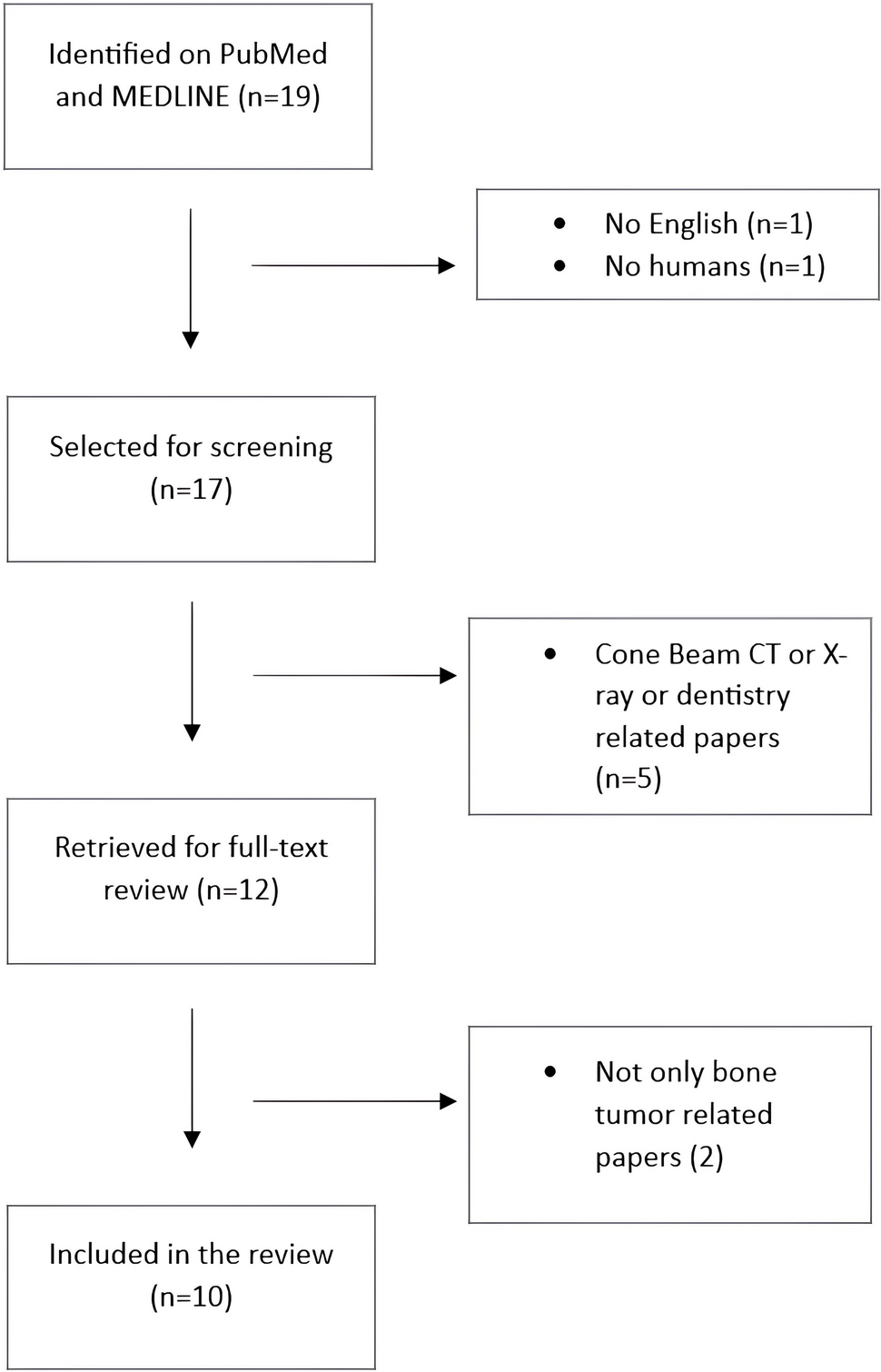
Screening the three databases (PubMed, Embase, Scopus) yielded a total of 1486 records, two of which were excluded because they were published before 2018; 357 duplicates were removed; 79 records lacked a DOI, making them unretrievable for full review. The remaining 1048 records were screened by title and abstract; 33 of the 36 selected for further analysis were excluded. The remaining 3 records met the inclusion criteria. Furthermore, other records gleaned from the references were identified as possibly relevant and were reviewed for eligibility via a search of citations. Three records were included in the systematic review (Fig. 2). The data were extracted, and two of us independently assessed the records for quality.
Quality assessmentQuality assessment was performed using a set of questions from the CASP method. The score was calculated as the percentage of criteria fulfilled, and the records were ranked accordingly (Fig. 3).
Fig. 3
In their correspondence, Berlyand et al. [9] reported evidence from a large reference dataset of studies to identify which AI interventions and subsequent operations can benefit emergency department workflow. A possible bias of the study was that author affiliation and geographical location of the evidence were the same. In their original research articles Chong et al. [10] and Verburg et al. [11] reported evidence from large patient datasets, with clear and concise methodologies. To conclude, the literature reviews [12,13,14] focused primarily on the future role of AI in the governance of radiology departments and the implications for healthcare professionals. Moreover, the studies analyzed how AI optimized workflow and clinical outcomes, with strong implications for management and organizational processes.
FindingsTable 3 presents an overview of the studies and details on AI applications. In detail, the studies were published between 2018 and 2022 with no predominance of any year and included literature reviews [12,13,14], original research articles, [10, 11] and correspondence. [9] All the studies discussed AI applied to radiology, both emergency radiology [9, 14] and elective radiology, [10,11,12,13] consistent with the inclusion criteria. The study on magnetic resonance imaging (MRI) as a diagnostic technique [10, 11] appeared relevant, as both original research articles investigated this. The stage in the care path in which AI is most often applied and investigated is appointment scheduling [10, 12, 13] and triaging. [9, 11]. Furthermore, the main types of AI were ML [9, 10, 12, 13] and DL. [11, 12]
Table 3 Study CharacteristicsCurrent AI admin solutions are generally employed to reduce fluctuations in healthcare demand, which are more prevalent in non-elective settings such as the emergency room. As a consequence, the focus was on triage and scheduling in admin AI.
Triage and patient stratificationOne benefit of AI for radiology departments is that it provides for faster interpretation of clinical data for patient classification during triage and clinical risk assessment during discharge [11, 13, 14]. Accurate and rapid triage based on highly sensitive algorithms can help to distinguish critically ill from stable patients [9] and predict response to therapy through “big data” data techniques, consisting of DL and other ML strategies. [12]
In addition, natural language processing (NLP) and ML models have been developed that can identify illnesses (e.g., sepsis, acute appendicitis, influenza) and perform computer-aided diagnosis with extraordinarily high accuracy using data typically available within hours of an emergency room visit. [9, 13] This type of analysis allows for better allocation and use of resources, patient management, and operations especially in urgent care. Such improvements allow for better matching of resources with patient needs, thus increasing efficiency in time and cost and improving patient outcomes. [9, 11, 12] Improvement in patient outcomes results from averting delays and potential worsening of illness, appropriately assigned resources, and data-backed care. Given the aging population in many developed countries and the rising costs of healthcare delivery, there is an imperative need to keep healthcare both accessible and affordable [10].
In addition, the workflow of specialists and the management of emergencies during elective appointment hours can benefit greatly from triage, faster risk stratification and identification. AI models can accurately predict wait times or appointment delays for computed tomography (CT), MRI, radiography, and ultrasound. The ability to communicate accurate waiting times to patients can improve patient satisfaction. [12]
Scheduling and workflowHospital outpatient appointment no-shows are a common problem and a costly burden to healthcare systems worldwide, as they contribute to inefficiencies and health access delays [10, 13]. Recent studies in appointment scheduling indicate that overtime, idle time, and patient waiting time can be substantially reduced by combining ML with a framework called predictive overbooking. [10, 15] In fact, ML techniques trained using high-dimensional datasets to produce complex high-performance predictive models can manage the multifaceted problem of appointment no-shows. [10] Moreover, studies agree that AI can benefit through worklist prioritization, double-checking of errors (i.e., misses), and predicting patient volume in the emergency department. [14, 16]
Furthermore, AI algorithms can be useful in providing guidance for selecting which imaging exam may be most appropriate (e.g., MRI rather than ultrasound based on patient characteristics). [12] Greater appropriateness of care and simultaneous reduction in idle time is likely to improve patient and staff satisfaction.
Claim and reimbursement processingMany variables can figure in a denied claim; AI can aid in coding and billing procedures. AI applications can positively impact on staff satisfaction in such tedious and repetitive tasks as medical coding. [12] For radiologists, less time spent on administrative tasks can free up time for diagnostics and patient care, both beneficial to clinical outcomes.
Comments (0)