Alkaptonuria, a rare metabolic disorder with a prevalence of 1 in 100,000 to 250,000, was first described by Sir Archibald Garrod in 1908 and follows autosomal recessive inheritance. [3] Common complications include spondylosis and arthropathies, with cardiac ochronosis being a notable but infrequent complication. [4] Despite over 60 case reports, [1] instances of cardiac ochronosis in Indian literature are sparse, underscoring the importance of accurate diagnosis.
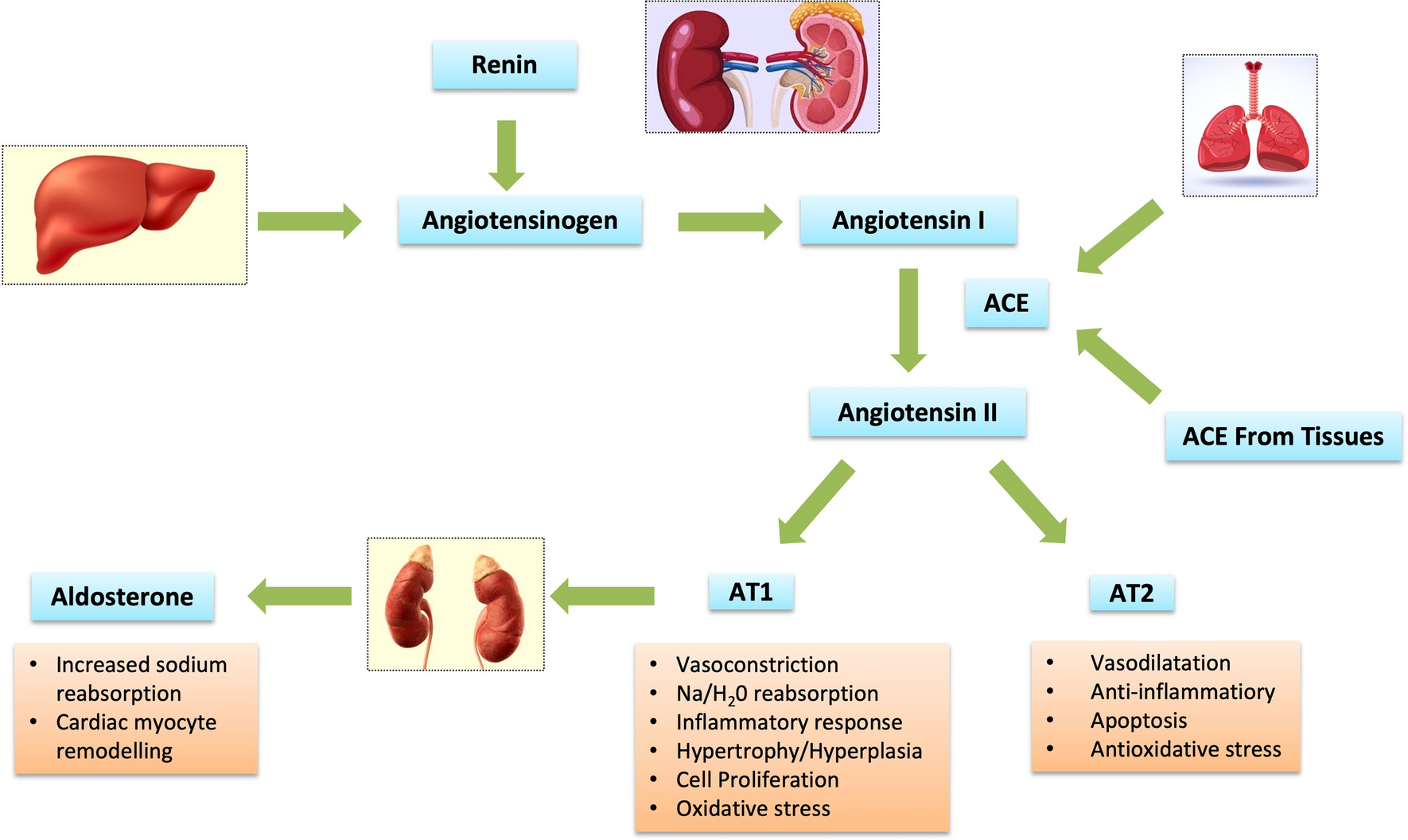
Apart from musculoskeletal involvement, alkaptonuria can present with various clinical manifestations, including ocular and cutaneous pigmentation, genitourinary obstruction due to ochronotic calculi, and cardiovascular involvement [4]. In the cardiovascular system, the calcified aortic valve is one of the most common sites for the deposition of black pigments. This phenomenon is more frequently observed in aortic stenosis than in aortic regurgitation, as calcific deposits are rarer in the latter. Hannoush et al. suggested that deposits of homogentisic acid can increase pressure or turbulence in vessels, damaging microvasculature and leading to dystrophic calcification. [5]
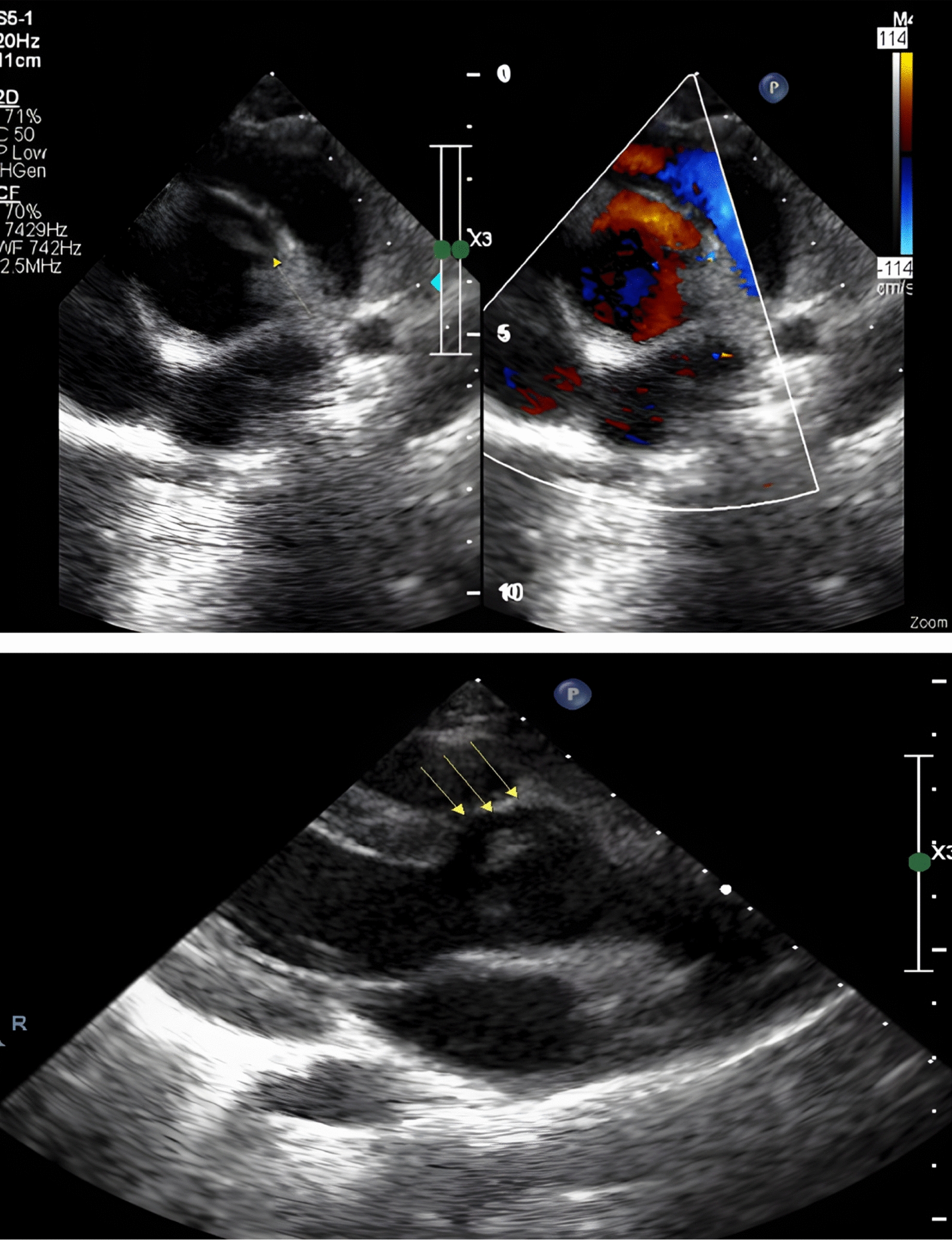
In our case, we observed characteristic black deposits in the aortic intima, including the aortic valve, which were identified intraoperatively. This finding was unexpected as the patient had not been previously diagnosed with alkaptonuria or exhibited symptoms suggestive of the condition. Consequently, the presence of ochronosis posed a dilemma for the predetermined surgical plan of replacing the aortic valve with a bioprosthetic valve. Given the lack of a confirmed diagnosis, differential diagnoses such as aortic dissection, intramural hematoma, or pigment disorders like hemochromatosis are needed to be considered. However, diagnostic modalities such as urine analysis for alkaptonuria and transesophageal echocardiography (TEE) clarified the situation and guided the surgical approach.
Although the patient initially preferred a bioprosthetic valve, we chose to use a mechanical valve due to concerns about potential pigmentation effects on a bioprosthetic valve [6] and the lack of long-term follow-up data on the incidence of paravalvular leaks and structural valve degeneration associated with bioprosthetic valves in cases of cardiac ochronosis. The hazardous effects of ochronosis on cardiac tissue remain unclear, and definitive therapeutic guidelines are yet to be established.
Ather and Roberts reviewed 66 cases of cardiac ochronosis, most of which involved the aorta. [1] While reports commonly document involvement of the aortic valve, there are also accounts of pigmentation affecting the mitral valve, aorta, internal mammary artery, and coronary arteries. Notably, in India, despite the high number of valve replacement surgeries performed, cases of cardiac ochronosis remain exceedingly rare.
Parashi et al. described a case involving alkaptonuric ochronosis of a congenital bicuspid aortic valve in a 38-year-old male patient with diagnosed alkaptonuria who was referred for valve replacement. [7] Their report highlighted the lack of standard guidelines for managing ochronotic valves and selecting prosthetic options. They opted for a mechanical valve due to the patient's age and concerns about the potential degeneration of a bioprosthetic valve caused by ochronosis.
Additionally, black pigmentation of the aortic valve and coronaries was observed in a post-liver transplant patient who underwent coronary bypass grafting and valve replacement with a bioprosthetic valve. In this case, the pigmentation was attributed to medications related to the transplant or changes in dysfunctional liver parenchyma, not alkaptonuria. The rationale for valve selection in this instance was not specified [7].
Reports of bioprosthetic valve replacement in alkaptonuria cases do exist [8, 9], and in those cases, the choice of valve was typically guided by general population guidelines. However, understanding how ochronotic deposits affect valve degeneration and function is crucial for informing future guidelines on prosthetic valve selection for affected patients. The current literature on the accelerated degeneration of biological prostheses and the impact of homogentisic acid (HGA) deposition on their durability is limited.
Although the surgery was uneventful and the patient was discharged without complications, she was advised to have regular follow-ups to assess valve gradients and monitor disease progression.




Comments (0)