
Remember me





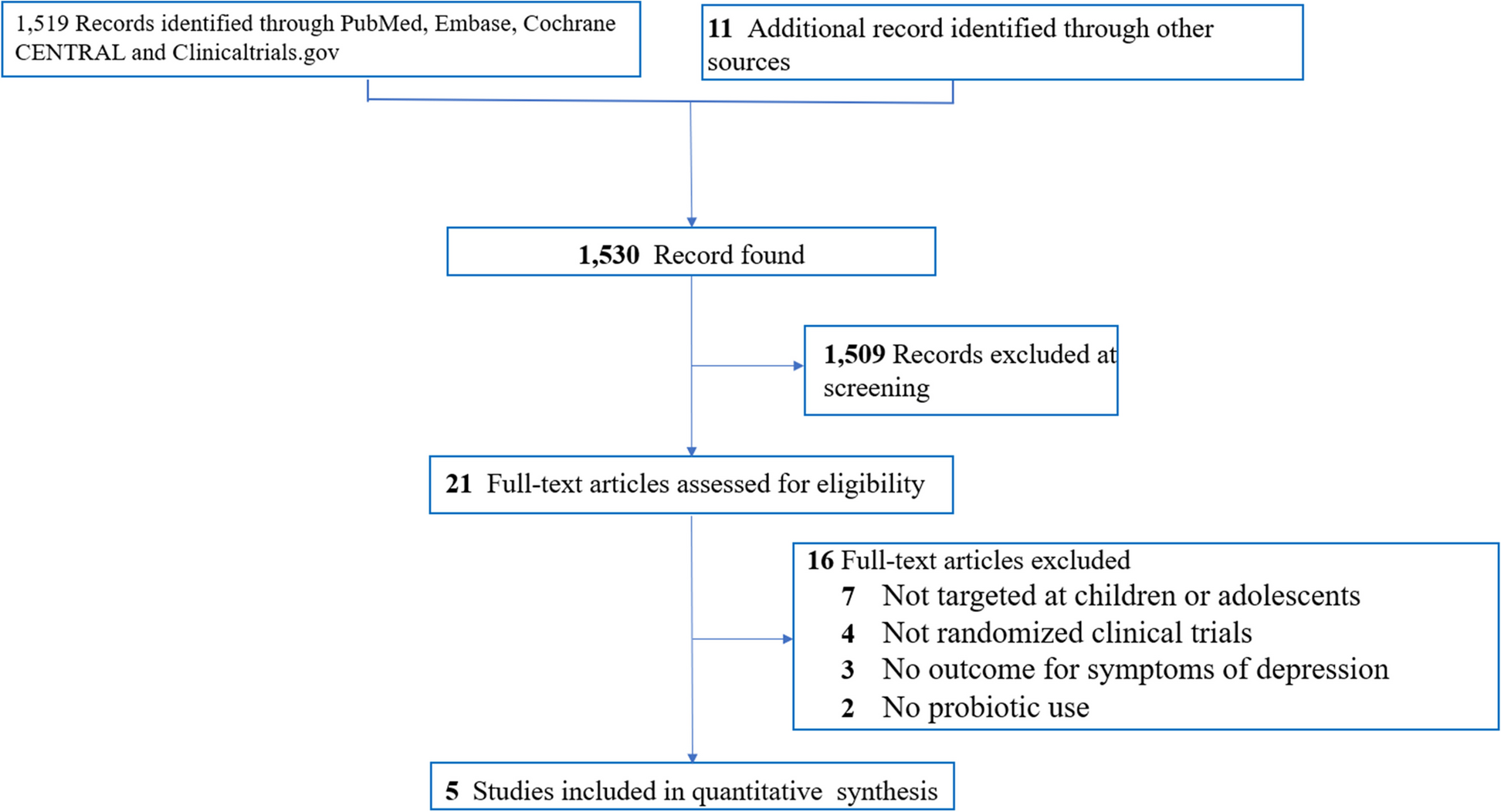


A total of 1494 studies were retrieved through electronic databases and University repositories. Fifty studies were excluded due to duplicates, giving 1444 studies. After the review of titles and abstracts, 1433 studies were excluded. Then one study was excluded for reason (not meeting the study target) [26]. We included ten full articles in this systematic review and meta-analysis (Fig. 1).
Characteristics of included studiesA total of 10 studies (nine published studies and one unpublished study) with a total 5812 of study participants which assessed the level of ICCM utilization and its predictors published /reported in the English language were included in this systematic review and meta-analysis.
The quality of the included studies was assessed using the NOS quality assessment tool and studies with a quality assessment score of ≥ 7 were considered as low risk for bias in this review [27](Supplementary file 2). With regards to the regional distributions, the included studies were conducted in South Ethiopia [14, 16], Southwest Ethiopia [19], Central Ethiopia [18, 22], Oromia [15, 20], Sidama Regions [17, 21], and Addis Ababa City Administration [23] (Table 2).
The prevalence of ICCM utilization based on individual studiesThe utilization of ICCM utilization was reported to be high in the study conducted by Bellete M. et al. [23] and Salgedo WB. et al. [19] with respective prevalence of 69.49% and 58.93%. Low ICCM utilization was reported in the study by Berhanu A.et al [14] and Rikiba R. et al. [21] with a prevalence of 10.43% and 18.20% respectively.
Meta-analysisThe level of integrated community case management of childhood illnesses (ICCM)Ten cross-sectional primary studies conducted in different regions of Ethiopia were used to compute the pooled level of ICCM utilization in Ethiopia [14,15,16,17,18,19,20,21,22,23]. In this study, the pooled level of ICCM utilization was found to be 42.73 (95%, CI 27.65%, 57.80%) (Fig. 2).
Fig. 2
The pooled prevalence of integrated community case management of childhood illnesses in Ethiopia
Sensitivity analysisWe conducted a sensitivity analysis to assess the influence of individual studies on the pooled prevalence of ICCM. Hence, the sensitivity analysis indicated that the point estimate of the individual study was within the confidence interval of the pooled prevalence (42.73%: 95%, CI 27.65%, 57.80%) which indicated no significant influence of individual studies (Fig. 3).
Fig. 3
Sensitivity analysis of included studies to estimate the pooled prevalence of ICCM in Ethiopia
Assessment of heterogeneity based on study site and sample sizeHigh heterogeneity was observed between primary studies used to determine the pooled level of ICCM utilization (Fig. 2). Subgroup analysis based on the study site and sample size were performed to diagnose the possible cause of heterogeneity (Figs. 4 and 5).
Fig. 4
Subgroup analysis of the level of integrated community case management of childhood illnesses in Ethiopia based on the study site
Fig. 5
Subgroup analysis of the level of integrated community case management of childhood illnesses in Ethiopia based on sample size
Subgroup analysis based on the study siteWith regards to the level of ICCM utilization, there was a significant difference between study sites with a test of group difference Q b1 value of 9.61 and p-value of < 0.001. The level of ICCM was 53.87% (95%, CI 40.66 -67.09%) and 25.73% (95%, CI 13.81, 37.64%) among studies done at community level and facility level respectively (Fig. 4).
Subgroup analysis based on sample sizeWe have used the sample mean to perform subgroup analysis based on sample size (sample size < 580 and ≥ 580). There is no significant difference in the level of ICCM between studies based on sample category with group difference test Q b1 value of 0.01 and p-value of 0.91. The level of ICCM utilization was found to be 43.64% (95%, CI 25.36%, 61.01%) and 41.73% (95%, CI 17.60%, 66.01%) among studies with sample size < 580 and studies with a sample size of ≥ 580 respectively (Fig. 5).
Assessment of publication biasFunnel plot and Egger’s asymmetry test were used to assess the presence of publication bias between primary studies. The funnel plot (Fig. 6) and Egger’s asymmetry test indicated no significant publication bias with a p-value of 0.157.
Fig. 6
Funnel plot of included studies in a meta-analysis of ICCM utilization in Ethiopia
Factors associated with the utilization of ICCM in EthiopiaIn this review, parents’ awareness about the illness, awareness about ICCM service, perceived severity of the disease, secondary/above level of education, and living within 30 min distance to the health post were variables significantly associated with utilization of ICCM in Ethiopia (Fig. 7).
Fig. 7
Forest plot of variables associated with utilization of ICCM in Ethiopia
There was a statistically significant association between parents’ awareness of illness and utilization of ICCM. The odds of utilizing ICCM service were found to be 2.77 higher among parents who have awareness about signs of illnesses compared to counterparts (OR = 2.77, 95%, CI 2.06, 3.74). Five primary studies were used to assess the association between awareness about signs of illnesses and ICCM utilization [15, 17, 19, 21, 23] with no significant heterogeneity between studies (I2 = 28.84%, P = 0.23). In the same manner, parents who have awareness about the availability of ICCM service were 3.64 times more likely to use ICCM service [14,15,16, 21, 22] compared to those who do not have awareness about the availability of ICCM service with moderate heterogeneity between primary studies (OR = 3.64, 95%, CI 2.16, 6.14, (I2 = 57.96%, P = 0.05)). (Fig. 7).
Perceived severity of diseases was found to be significantly associated with ICCM utilization compared to counterparts [16, 17, 23]. The odds of ICCM utilization were found to be3.14 times higher among those who had high perceived severity about diseases compared to counterparts with no heterogeneity between primary studies (OR = 3.14, 95%, CI 2.33, 4.23), I2 = 0.00%, P = 0.77). Parents’ level of education was also found to be significantly associated with ICCM utilization based on pooled evidence from three primary studies. Parents with secondary or above level of education were 2.57 times more likely to utilize ICCM for their sick children compared to counterparts (OR = 2.57, 95%, CI 1.39, 4.77), I2 = 57.57%, P = 0.09) with minor heterogeneity between primary studies. Similarly, those who lived within 30 min distance of the health post were 3.93 times more likely to use ICCM service compared to those who live in areas more than 30 min away from a health post (OR = 3.93, 95%, CI 2.30, 6.74) with no significant heterogeneity( I2 = 27.16, P = 0.25 ) between primary studies [14, 16, 19, 21] (Fig. 7).
Comments (0)