
Remember me





This will be a multi-site, two-armed, parallel-group, single-blind, superiority randomised controlled trial investigating the physiological and psychological effects of a telehealth-delivered 16-week aerobic and resistance exercise intervention in a biventricular congenital heart cohort, employing pre- and post-intervention measurements, with an 8-month follow-up.
Trial setting and sitesRecruitment will occur at the Royal Prince Alfred Hospital, Royal Melbourne Hospital, Prince Charles Hospital, and Fiona Stanley Hospital in Australia. Potential recruits will be identified from the National Congenital Heart Disease Registry and trial site cardiologists. We include multiple sites in order to enhance participant enrolment and reach our target sample size.
ParticipantsMedical records and telephone screening will be used to determine if potential recruits fulfil trial eligibility criteria. Treating or study physicians will confirm the suitability of potential recruits to enrol in the trial. Trial team members have consulted with various consumer organisations comprising individuals and their families with lived experience of congenital heart conditions while designing the trial, and this is expected to positively affect participant recruitment numbers. Additionally, information about the trial as well as participant information and recruitment material will be placed on institutional and study partner social media platforms and websites. A dedicated website page (https://www.hri.org.au/ch-fit-online-registrations) has been created where individuals can register their interest to participate and who can then be triaged to their nearest trial site.
Inclusion criteriaPatients 16–55 years with biventricular congenital heart conditions of varying complexity, physiological stage B-C according to International Guidelines [40], and medically stable, who are > 6 months post-cardiac surgery as identified at the listed participating sites, and who may also present with conditions such as repaired tetralogy of Fallot and transposition of the great arteries, will be included. We have kept our inclusion criteria broad in order to achieve adequate participant enrolment.
Exclusion criteriaExclusion is (1) based on the last cardiologist’s assessment present in the recruit’s medical record and (2) determined at pre-intervention exercise testing. Exclusion criteria include simple lesion without sequelae such as a small ventricular septal defect, severe active enlargement of aorta, poorly controlled arrhythmias/blood pressure prior to or during exercise, non-optimal medical therapy and clinically unstable conditions in the preceding 3 months, severe outflow tract obstruction, severe valvular regurgitation, and uncontrolled systemic hypertension or decompensated heart failure (New York Heart Association (NYHA) class IV).
Further exclusion criteria include a physiological stage of D (severe hypoxaemia, systemic level pulmonary hypertension, Eisenmenger syndrome, refractory end-organ dysfunction) [40] as well as intellectual and/or physical disability preventing self-directed exercise, pregnancy or planned pregnancy (within 12 months), planned surgical intervention (within 2 years), self-reported volumes of PA or exercise sufficient to meet current minimum PA and exercise guidelines, and/or with no or an unreliable Internet connection. Our exclusion criteria aim to minimise the possibility of adverse or serious adverse events occurring, while still allowing for a broad recruitment strategy.
Participant consent and withdrawalWritten, informed consent will be obtained at baseline visits, prior to assessment and randomisation, by site staff. Should an enrolled participant withdraw during the trial, they will be requested to complete a withdrawal form. Data collected from these participants will be retained for intention-to-treat analysis where consent is provided to retain data. Additional written, informed consent pertaining to outcomes requiring the collection of biological specimens via venesection and/or cannulation will also be obtained.
Power analysis and statistical measuresA sample size of 100 is predicted to have ≥ 90% power (two-sided α: 5%) in estimating a VO2peak difference of 10% between intervention and control (primary outcome), as suggested by preliminary findings [41]. We assume a 10% drop-out for a 16-week duration. Generalised linear mixed models with random subject and site effects (to control for variation between individuals and the clustering effects of site) and group-time interactions will be used to estimate the between and within group pre- and post-intervention changes in the primary outcome, controlling for covariates that may influence the outcome. Results will be summarised using descriptive and inferential statistics, with relevant P values (significance < 0.05). Sensitivity analysis of per-protocol vs intention-to-treat will be conducted. We will handle missing data by imputation using the closest match method. i.e. substitute a same time-point value from a participant with the closest value for the measured variable at other time points [42].
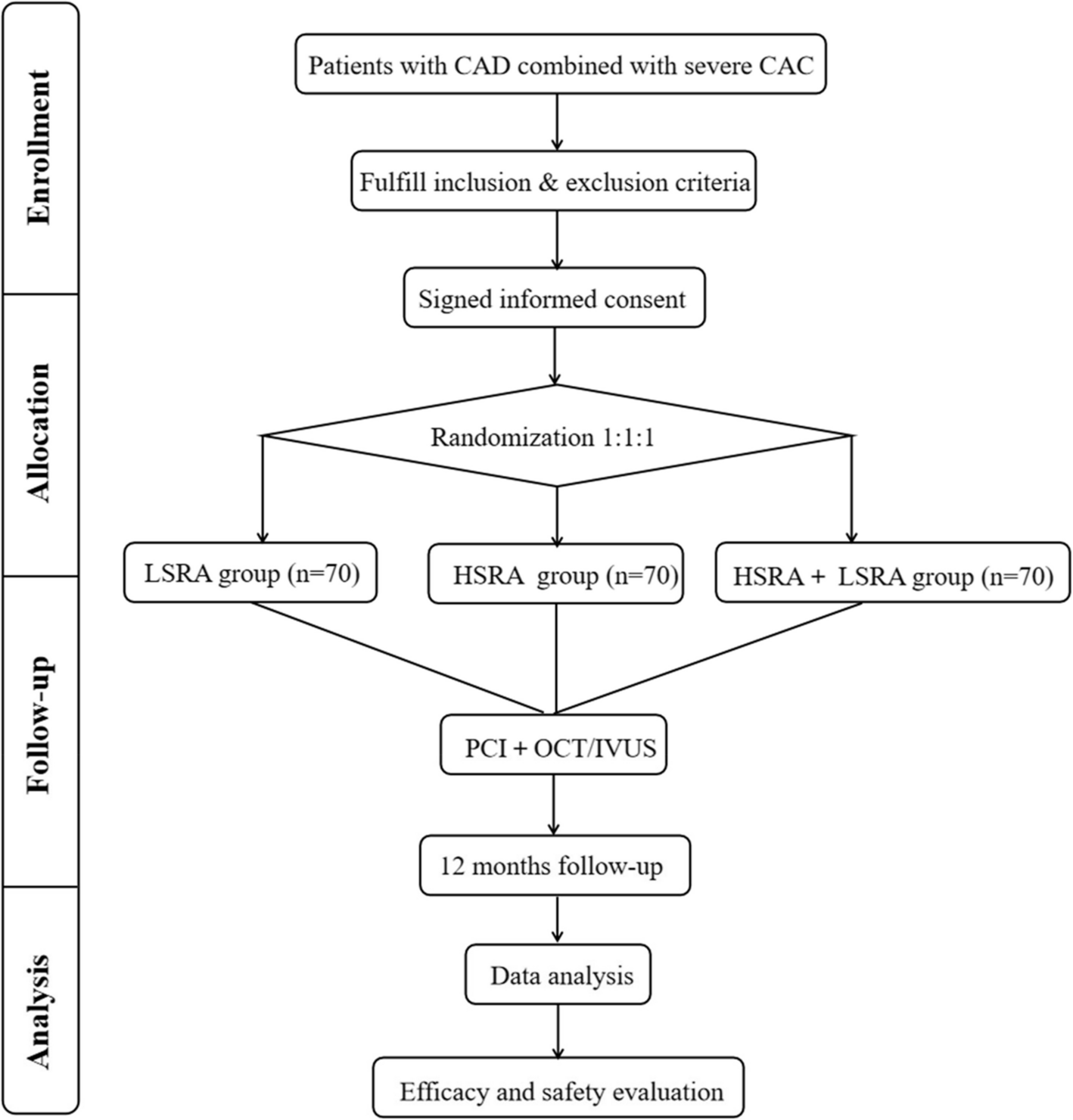
Randomisation and concealmentComputer-generated randomisation will be stratified on a 1:1 allocation by site, baseline aerobic exercise capacity (% predicted VO2peak), physiological stage (B or C), age, and sex (female, male), per Fig. 1. An independent statistician/staff member will employ randomisation by minimisation to allocate participants. Where possible, site assessors will be blinded to participant group allocation and identification. Participants’ data and identification will be stored centrally (REDCap™) and accessible only by a trial coordinator (uninvolved in participant enrolment, randomisation, or assessment). Unblinding is expected to occur in the event of a serious adverse or adverse event. Participants are not blinded owing to the nature of the intervention (exercise).
Fig. 1
The Congenital Heart Fitness Intervention Trial (CH-FIT) study design flow chart
Flow of participants (recruitment to completion) and scheduleFigure 1 presents the study design flow chart of participants, and Table 1 lists the schedule of recruitment, consent, enrolment, assessments, randomisation, intervention, and follow-up periods. The recruitment period is expected to last for approximately 30 months, with an expected monthly rate of recruitment commensurate with each site’s participant allocation (generally 3–4 participants per month across all sites). In addition, sites will over-recruit by up to 10% in order to achieve sufficient participant enrolment to attain the required adequately powered sample size.
Table 1 The Congenital Heart Fitness Intervention Trial (CH-FIT) schedule of visits (Tables 3 and 4 )For each trial site, the target sample size is summarised in Table 2.
Table 2 Participant numbers (intervention and control) per trial site
Comments (0)